- Page 3:
PrefaceIn the region of Central and
- Page 8 and 9:
Practical Lab MaterialsAirway .....
- Page 11 and 12:
Guidelines for Conducting the First
- Page 13 and 14:
sheets supplied in this guide will
- Page 15 and 16:
should have attended a workshop tha
- Page 17 and 18:
Job Description: First ResponderThe
- Page 19:
c. Additional Skills1. Use of the t
- Page 22 and 23:
as possible. After students have pr
- Page 25 and 26:
Guidelines for Case-Based Practical
- Page 27 and 28:
General Lecturing GuidelinesChapter
- Page 29:
discussing the different methods of
- Page 32 and 33:
survival. First Responders include
- Page 34 and 35:
medical director functions to ensur
- Page 37 and 38:
First Responder EMS Curriculum/AIHA
- Page 39 and 40:
First Responder EMS Curriculum/AIHA
- Page 41 and 42:
Well-Being of the First ResponderCo
- Page 43 and 44:
and family. Do not become defensive
- Page 45 and 46:
1. Eye protection. Safety glasses m
- Page 47 and 48:
First Responder EMS Curriculum/AIHA
- Page 49 and 50:
First Responder EMS Curriculum/AIHA
- Page 51 and 52:
Legal and Ethical IssuesContents1.
- Page 53 and 54:
a. Expressed ConsentExpressed conse
- Page 55 and 56:
14. DocumentationProviding written
- Page 57 and 58:
First Responder EMS Curriculum/AIHA
- Page 59 and 60:
First Responder EMS Curriculum/AIHA
- Page 61 and 62:
The Human Body: A Systems ApproachC
- Page 63 and 64:
that the pharynx performs the dual
- Page 65:
c. Kinesthetic (Doing)1. Students w
- Page 68 and 69:
38 First Responder EMS Curriculum/A
- Page 70 and 71:
40 First Responder EMS Curriculum/A
- Page 72 and 73:
42 First Responder EMS Curriculum/A
- Page 75 and 76:
Lifting and Moving PatientsContents
- Page 77 and 78:
If the patient is on the floor or g
- Page 79 and 80:
7. Application of Content Materiala
- Page 81 and 82:
First Responder EMS Curriculum/AIHA
- Page 83 and 84:
First Responder EMS Curriculum/AIHA
- Page 85 and 86:
First Responder EMS Curriculum/AIHA
- Page 87 and 88:
First Responder EMS Curriculum/AIHA
- Page 89:
First Responder EMS Curriculum/AIHA
- Page 92 and 93:
14. Describe how to clear a foreign
- Page 94 and 95:
Precautions1. Finger must not press
- Page 96 and 97:
. Finger SweepsThis method involves
- Page 98 and 99:
4. Place your other fingers along t
- Page 100 and 101:
. Management of the Obstructed Airw
- Page 102 and 103:
5. Students will practice ventilati
- Page 104 and 105:
74 First Responder EMS Curriculum/A
- Page 106 and 107:
76 First Responder EMS Curriculum/A
- Page 108 and 109:
78 First Responder EMS Curriculum/A
- Page 110 and 111:
19. Explain what additional questio
- Page 112 and 113:
can be determined by questioning th
- Page 114 and 115:
Determine estimated time of arrival
- Page 116 and 117:
E - Events Leading to the Injury or
- Page 118 and 119:
c. Kinesthetic (Doing)1. Students w
- Page 120 and 121:
90 First Responder EMS Curriculum/A
- Page 122 and 123:
92 First Responder EMS Curriculum/A
- Page 124 and 125:
94 First Responder EMS Curriculum/A
- Page 126 and 127:
96 First Responder EMS Curriculum/A
- Page 128 and 129:
98 First Responder EMS Curriculum/A
- Page 130 and 131:
100 First Responder EMS Curriculum/
- Page 133 and 134:
CirculationContents1. Objectivesa.
- Page 135 and 136:
Veins are the vessels that carry bl
- Page 137 and 138:
Step 5:Step 6:Step 7:Step 8:Step 9:
- Page 139 and 140:
Steps of Infant CPRStep 1: Assess r
- Page 141 and 142:
a. Use of the Semiautomatic Externa
- Page 143:
PracticalEvaluate the actions of th
- Page 146 and 147:
116 First Responder EMS Curriculum/
- Page 148 and 149:
118 First Responder EMS Curriculum/
- Page 150 and 151:
120 First Responder EMS Curriculum/
- Page 153 and 154:
Medical EmergenciesContents1. Objec
- Page 155 and 156:
5. Demonstrate the steps in providi
- Page 157 and 158:
additional emergency medical person
- Page 159 and 160:
this internal temperature, adverse
- Page 161 and 162:
Signs and SymptomsSigns and symptom
- Page 163 and 164:
3. Ask questions in a calm, reassur
- Page 165:
EvaluationWrittenDevelop evaluation
- Page 168 and 169:
138 First Responder EMS Curriculum/
- Page 170 and 171:
140 First Responder EMS Curriculum/
- Page 172 and 173:
142 First Responder EMS Curriculum/
- Page 174 and 175:
144 First Responder EMS Curriculum/
- Page 176 and 177:
146 First Responder EMS Curriculum/
- Page 178 and 179:
148 First Responder EMS Curriculum/
- Page 180 and 181:
150 First Responder EMS Curriculum/
- Page 182 and 183:
152 First Responder EMS Curriculum/
- Page 184 and 185:
154 First Responder EMS Curriculum/
- Page 186 and 187:
2. Attend to the feelings of the pa
- Page 188 and 189:
transmission of disease to yourself
- Page 190 and 191:
Sharp, pointed objects cause penetr
- Page 192 and 193:
c. Chemical BurnsChemical burns fro
- Page 194 and 195:
6. Partial-thickness burns7. Full-t
- Page 196 and 197:
166 First Responder EMS Curriculum/
- Page 198 and 199:
168 First Responder EMS Curriculum/
- Page 200 and 201:
170 First Responder EMS Curriculum/
- Page 202 and 203:
172 First Responder EMS Curriculum/
- Page 204 and 205:
2. Demonstrate opening the airway i
- Page 206 and 207:
3. Try to pad the extremity to prev
- Page 208 and 209:
soft tissue injuries. Remember, the
- Page 211 and 212:
First Responder EMS Curriculum/AIHA
- Page 213 and 214:
First Responder EMS Curriculum/AIHA
- Page 215 and 216:
First Responder EMS Curriculum/AIHA
- Page 217 and 218:
First Responder EMS Curriculum/AIHA
- Page 219:
First Responder EMS Curriculum/AIHA
- Page 222 and 223:
2. IntroductionChildbirth can occur
- Page 224 and 225:
a. Delivery ProceduresWhen assistin
- Page 226 and 227:
5. Student Activitiesa. Auditory (H
- Page 228 and 229:
198 First Responder EMS Curriculum/
- Page 230 and 231:
200 First Responder EMS Curriculum/
- Page 232 and 233:
202 First Responder EMS Curriculum/
- Page 235 and 236:
Infants and ChildrenContents1. Obje
- Page 237 and 238:
Suctioning the airway also is an im
- Page 239 and 240:
6. Common Problems in Infants and C
- Page 241 and 242:
Remember that parents will be in ag
- Page 243 and 244:
Vigorous shaking of a baby may show
- Page 245 and 246:
First Responder EMS Curriculum/AIHA
- Page 247 and 248:
First Responder EMS Curriculum/AIHA
- Page 249 and 250:
First Responder EMS Curriculum/AIHA
- Page 251 and 252:
First Responder EMS Curriculum/AIHA
- Page 253:
First Responder EMS Curriculum/AIHA
- Page 256 and 257:
3. DispatchDispatch is the communic
- Page 258 and 259:
in the absence of airway problems,
- Page 261 and 262:
First Responder EMS Curriculum/AIHA
- Page 263 and 264:
First Responder EMS Curriculum/AIHA
- Page 265 and 266:
Documentation and Quality Managemen
- Page 267 and 268:
Identify concrete, specific project
- Page 269 and 270:
First Responder EMS Curriculum/AIHA
- Page 271 and 272:
First Responder EMS Curriculum/AIHA
- Page 273 and 274:
Practical Lab: AirwayObjectives1. C
- Page 275:
6. Students will practice insertion
- Page 278 and 279:
Assistant Instructor:The instructor
- Page 281 and 282:
Practical Lab: CirculationObjective
- Page 283 and 284:
Practical Lab: Illness and InjuryOb
- Page 285 and 286:
Instructor will demonstrate the pro
- Page 287:
19. Students will practice manual s
- Page 290 and 291:
Assistant InstructorThe instructor-
- Page 293 and 294:
Practical Lab: Lifting and Moving P
- Page 295:
EvaluationPracticalEvaluate the act
- Page 298 and 299:
4. Insert it posteriorly. Bevel sho
- Page 300 and 301:
• 20 breaths per minute for child
- Page 302 and 303:
one per second, each with the inten
- Page 305 and 306:
Skill Descriptions: Patient Assessm
- Page 307 and 308:
Skill Descriptions: CirculationNote
- Page 309 and 310:
4. To determine whether the victim
- Page 311 and 312:
• Place the two fingers of one ha
- Page 313 and 314:
Skill Descriptions: Illness and Inj
- Page 315:
• Apply enough pressure to contro
- Page 318 and 319:
12. As the feet are delivered, gras
- Page 320 and 321:
2. The rescuer at the head places o
- Page 322 and 323:
Skill Algorithms: AirwayForeign Bod
- Page 325 and 326: Trauma PatientSkill Algorithms: Pat
- Page 327: Skill Algorithms: Patient Assessmen
- Page 330 and 331: Two-Person CPRSkill Algorithms: Cir
- Page 333 and 334: External BleedingSkill Algorithms:
- Page 335: Skill Algorithms: Illness and Injur
- Page 338 and 339: Skill Algorithms: Childbirth and Ch
- Page 341 and 342: Skill Algorithms: Lifting and Movin
- Page 343: Skill Algorithms: Lifting and Movin
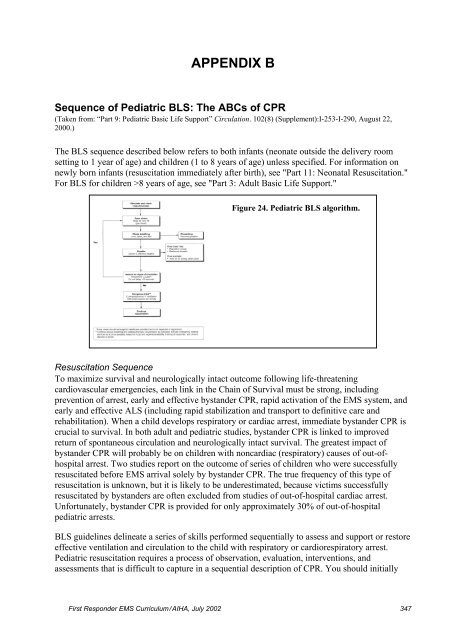
- Page 347: Sample Case Scenario - Patient Asse
- Page 351 and 352: Sample Case Scenario - Illness and
- Page 353: Sample Case Scenario - Childbirth a
- Page 356 and 357: • Demonstrate the extremity lift.
- Page 358 and 359: Figure 6. Check for unresponsivenes
- Page 360 and 361: Head Tilt-Chin Lift ManeuverTo acco
- Page 362 and 363: help. Monitor the victim, particula
- Page 364 and 365: necessary to open the victim's mout
- Page 366 and 367: In the second technique (lateral te
- Page 368 and 369: is important to note that this smal
- Page 370 and 371: CirculationAssessment: No Pulse Che
- Page 372 and 373: these arteries even when hypotensio
- Page 374 and 375: the nipples. This method has been u
- Page 378 and 379: assess the victim's responsiveness
- Page 380 and 381: arrhythmias should be instructed to
- Page 382 and 383: jaw lift, for use in unresponsive v
- Page 384 and 385: Figure 29. Mouth-to-mouth breathing
- Page 386 and 387: Types of Ventilation Bags (Manual R
- Page 388 and 389: Gastric Inflation. Increasing inspi
- Page 390 and 391: . Specificity (ability to correctly
- Page 392 and 393: After provision of approximately 20
- Page 394 and 395: Chest Compression in the Infant (<
- Page 396 and 397: ventilation after every fifth compr
- Page 398 and 399: Coordination of Compressions and Re
- Page 400 and 401: necessary to maintain optimal venti
- Page 402 and 403: 5. Keep foreign objects (i.e., marb
- Page 404 and 405: Figure 38. Subdiaphragmaticabdomina
- Page 406 and 407: tongue. Then use a hooking action t
- Page 409 and 410: APPENDIX DRelief of Foreign-Body Ai
- Page 411 and 412: Figure 41. Infant back blows to rel
- Page 413: 4. Repeat steps 1 through 3 until t
- Page 416 and 417: 6. It may be necessary for the Firs
- Page 418 and 419: 18. The correct rate to deliver che
- Page 420 and 421: 30. What is the greatest danger to
- Page 423 and 424: First Responder Post-Course Test1.
- Page 425 and 426: 12. Which of the following statemen
- Page 427 and 428:
24. Components of an ongoing assess
- Page 429 and 430:
36. An adult patient sustains burns
- Page 431:
48. Which of the following is true?
- Page 435 and 436:
First Responder Extra Test Question
- Page 437 and 438:
11. Negligence is the deviation fro
- Page 439 and 440:
Answer KeyFirst Responder Extra Tes