

PDF (5 MB) - Jurnalul de Chirurgie
PDF (5 MB) - Jurnalul de Chirurgie
PDF (5 MB) - Jurnalul de Chirurgie

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
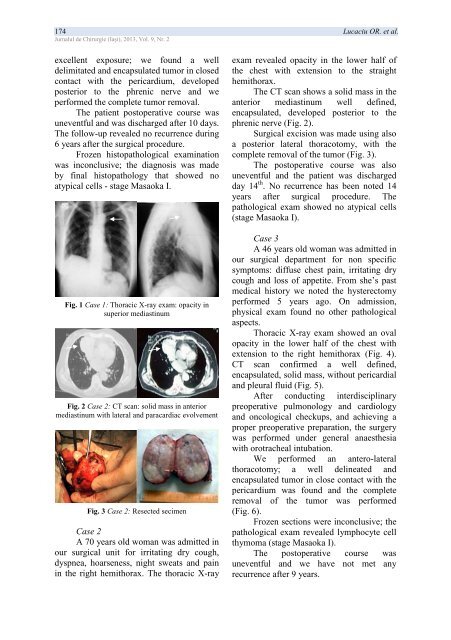
174 Lucaciu OR. et al.<strong>Jurnalul</strong> <strong>de</strong> <strong>Chirurgie</strong> (Iaşi), 2013, Vol. 9, Nr. 2excellent exposure; we found a well<strong>de</strong>limitated and encapsulated tumor in closedcontact with the pericardium, <strong>de</strong>velopedposterior to the phrenic nerve and weperformed the complete tumor removal.The patient postoperative course wasuneventful and was discharged after 10 days.The follow-up revealed no recurrence during6 years after the surgical procedure.Frozen histopathological examinationwas inconclusive; the diagnosis was ma<strong>de</strong>by final histopathology that showed noatypical cells - stage Masaoka I.Fig. 1 Case 1: Thoracic X-ray exam: opacity insuperior mediastinumFig. 2 Case 2: CT scan: solid mass in anteriormediastinum with lateral and paracardiac evolvementFig. 3 Case 2: Resected secimenCase 2A 70 years old woman was admitted inour surgical unit for irritating dry cough,dyspnea, hoarseness, night sweats and painin the right hemithorax. The thoracic X-rayexam revealed opacity in the lower half ofthe chest with extension to the straighthemithorax.The CT scan shows a solid mass in theanterior mediastinum well <strong>de</strong>fined,encapsulated, <strong>de</strong>veloped posterior to thephrenic nerve (Fig. 2).Surgical excision was ma<strong>de</strong> using alsoa posterior lateral thoracotomy, with thecomplete removal of the tumor (Fig. 3).The postoperative course was alsouneventful and the patient was dischargedday 14 th . No recurrence has been noted 14years after surgical procedure. Thepathological exam showed no atypical cells(stage Masaoka I).Case 3A 46 years old woman was admitted inour surgical <strong>de</strong>partment for non specificsymptoms: diffuse chest pain, irritating drycough and loss of appetite. From she’s pastmedical history we noted the hysterectomyperformed 5 years ago. On admission,physical exam found no other pathologicalaspects.Thoracic X-ray exam showed an ovalopacity in the lower half of the chest withextension to the right hemithorax (Fig. 4).CT scan confirmed a well <strong>de</strong>fined,encapsulated, solid mass, without pericardialand pleural fluid (Fig. 5).After conducting interdisciplinarypreoperative pulmonology and cardiologyand oncological checkups, and achieving aproper preoperative preparation, the surgerywas performed un<strong>de</strong>r general anaesthesiawith orotracheal intubation.We performed an antero-lateralthoracotomy; a well <strong>de</strong>lineated an<strong>de</strong>ncapsulated tumor in close contact with thepericardium was found and the completeremoval of the tumor was performed(Fig. 6).Frozen sections were inconclusive; thepathological exam revealed lymphocyte cellthymoma (stage Masaoka I).The postoperative course wasuneventful and we have not met anyrecurrence after 9 years.













