GTMB 7 - Gene Therapy & Molecular Biology
GTMB 7 - Gene Therapy & Molecular Biology
GTMB 7 - Gene Therapy & Molecular Biology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
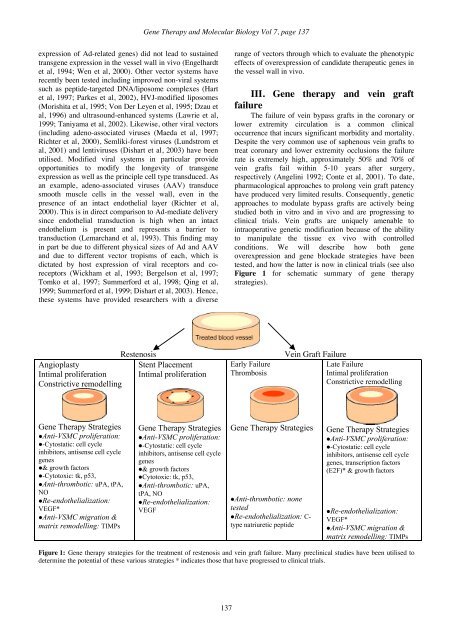
<strong>Gene</strong> <strong>Therapy</strong> and <strong>Molecular</strong> <strong>Biology</strong> Vol 7, page 137expression of Ad-related genes) did not lead to sustainedtransgene expression in the vessel wall in vivo (Engelhardtet al, 1994; Wen et al, 2000). Other vector systems haverecently been tested including improved non-viral systemssuch as peptide-targeted DNA/liposome complexes (Hartet al, 1997; Parkes et al, 2002), HVJ-modified liposomes(Morishita et al, 1995; Von Der Leyen et al, 1995; Dzau etal, 1996) and ultrasound-enhanced systems (Lawrie et al,1999; Taniyama et al, 2002). Likewise, other viral vectors(including adeno-associated viruses (Maeda et al, 1997;Richter et al, 2000), Semliki-forest viruses (Lundstrom etal, 2001) and lentiviruses (Dishart et al, 2003) have beenutilised. Modified viral systems in particular provideopportunities to modify the longevity of transgeneexpression as well as the principle cell type transduced. Asan example, adeno-associated viruses (AAV) transducesmooth muscle cells in the vessel wall, even in thepresence of an intact endothelial layer (Richter et al,2000). This is in direct comparison to Ad-mediate deliverysince endothelial transduction is high when an intactendothelium is present and represents a barrier totransduction (Lemarchand et al, 1993). This finding mayin part be due to different physical sizes of Ad and AAVand due to different vector tropisms of each, which isdictated by host expression of viral receptors and coreceptors(Wickham et al, 1993; Bergelson et al, 1997;Tomko et al, 1997; Summerford et al, 1998; Qing et al,1999; Summerford et al, 1999; Dishart et al, 2003). Hence,these systems have provided researchers with a diverserange of vectors through which to evaluate the phenotypiceffects of overexpression of candidate therapeutic genes inthe vessel wall in vivo.III. <strong>Gene</strong> therapy and vein graftfailureThe failure of vein bypass grafts in the coronary orlower extremity circulation is a common clinicaloccurrence that incurs significant morbidity and mortality.Despite the very common use of saphenous vein grafts totreat coronary and lower extremity occlusions the failurerate is extremely high, approximately 50% and 70% ofvein grafts fail within 5-10 years after surgery,respectively (Angelini 1992; Conte et al, 2001). To date,pharmacological approaches to prolong vein graft patencyhave produced very limited results. Consequently, geneticapproaches to modulate bypass grafts are actively beingstudied both in vitro and in vivo and are progressing toclinical trials. Vein grafts are uniquely amenable tointraoperative genetic modification because of the abilityto manipulate the tissue ex vivo with controlledconditions. We will describe how both geneoverexpression and gene blockade strategies have beentested, and how the latter is now in clinical trials (see alsoFigure 1 for schematic summary of gene therapystrategies).AngioplastyIntimal proliferationConstrictive remodellingRestenosisStent PlacementIntimal proliferationEarly FailureThrombosisVein Graft FailureLate FailureIntimal proliferationConstrictive remodelling<strong>Gene</strong> <strong>Therapy</strong> StrategiesAnti-VSMC proliferation:-Cytostatic: cell cycleinhibitors, antisense cell cyclegenes& growth factors-Cytotoxic: tk, p53,Anti-thrombotic: uPA, tPA,NORe-endothelialization:VEGF*Anti-VSMC migration &matrix remodelling: TIMPs<strong>Gene</strong> <strong>Therapy</strong> StrategiesAnti-VSMC proliferation:-Cytostatic: cell cycleinhibitors, antisense cell cyclegenes& growth factorsCytotoxic: tk, p53,Anti-thrombotic: uPA,tPA, NORe-endothelialization:VEGF<strong>Gene</strong> <strong>Therapy</strong> StrategiesAnti-thrombotic: nonetestedRe-endothelialization: C-type natriuretic peptide<strong>Gene</strong> <strong>Therapy</strong> StrategiesAnti-VSMC proliferation:-Cytostatic: cell cycleinhibitors, antisense cell cyclegenes, transcription factors(E2F)* & growth factorsRe-endothelialization:VEGF*Anti-VSMC migration &matrix remodelling: TIMPsFigure 1: <strong>Gene</strong> therapy strategies for the treatment of restenosis and vein graft failure. Many preclinical studies have been utilised todetermine the potential of these various strategies * indicates those that have progressed to clinical trials.137