

Sabato 27 ottobre 2012 - Pacini Editore
Sabato 27 ottobre 2012 - Pacini Editore
Sabato 27 ottobre 2012 - Pacini Editore

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
368<br />
Fig. 1. Gross appearance of the Wdpm: a whitish rough plaque with<br />
papillae easily detectable on cut surface.<br />
within the opened specimen. Histological examination showed a<br />
chronic follicular cholecystitis. Aspecific findings suggestive for<br />
prior surgical abdominal interventions, such as numerous foamy<br />
histiocytes (CD68+), steatonecrosis, fibrosis and mild chronic inflammation<br />
were noted on the epiploic appendix and on the hard<br />
fibrous nodule containing the Prolene implant, the latter probably<br />
representing a hernioplastic plug migrated from the inguinal canal<br />
and endoved within the abdominal cavity. Microscopic examination<br />
of the omental peritoneal lesion showed a papillary proliferation<br />
consisting of thick prominent sclerohyaline cores lined by a<br />
single row of bland cuboidal mesothelial cells. Immunoperoxydase<br />
studies demonstrated that the lining cells were positive for<br />
CK 5/6 and calretinin, thus confirming their mesothelial nature<br />
(Fig. 2). No mitotic activity, multistratification or significative<br />
cytological atypia were present. Electron microscopic examination<br />
further confirmed the mesothelial nature of the cells lining<br />
the papillary proliferation and their bland cytological ultrastructural<br />
features consisting of microvilli, rough endoplasmic reticulum,<br />
microfilaments, and desmosomes (Fig. 3), in keeping with<br />
previously reported findings 1 . According to the aforementioned<br />
histological, immunohistochemical and ultrastructural features, a<br />
diagnosis of WDPM was made.<br />
In consideration of the substantial benignity of this entity, as<br />
reported in the literature, in contrast to malignant mesothelioma<br />
Fig. 2. Histological features of the lesion, consisting of thick, sclerotic<br />
papillae lined by a single row of non atypical mesothelial cells. a. low<br />
magnification (2x, H&E); B. detail of the papillae with a thick fibrovascular<br />
cores (10x, H&E); C. positive immunohistochemical staining for<br />
Calretinin; d. positive immunohistochemical staining for Ck5/6.<br />
CONGRESSO aNNualE di aNatOmia patOlOGiCa SiapEC – iap • fiRENzE, 25-<strong>27</strong> OttOBRE <strong>2012</strong><br />
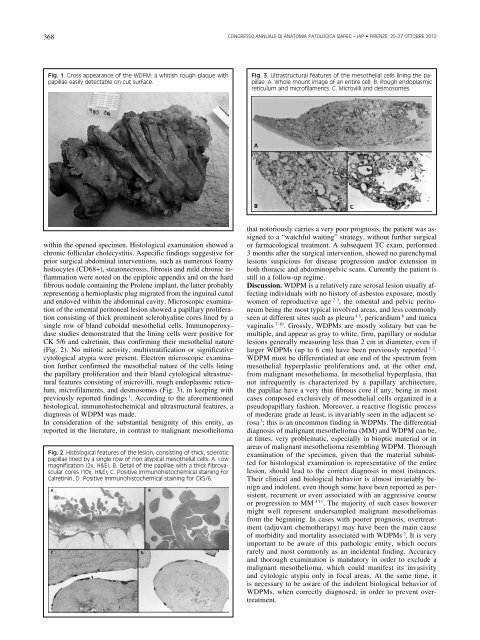
Fig. 3. ultrastructural features of the mesothelial cells lining the papillae.<br />
a. Whole mount image of an entire cell; B. Rough endoplasmic<br />
reticulum and microfilaments. c. Microvilli and desmosomes.<br />
that notoriously carries a very poor prognosis, the patient was assigned<br />
to a “watchful waiting” strategy, without further surgical<br />
or farmacological treatment. A subsequent TC exam, performed<br />
3 months after the surgical intervention, showed no parenchymal<br />
lesions suspicious for disease progression and/or extension in<br />
both thoracic and abdominopelvic scans. Currently the patient is<br />
still in a follow-up regime.<br />
Discussion. WDPM is a relatively rare serosal lesion usually affecting<br />
individuals with no history of asbestos exposure, mostly<br />
women of reproductive age 2 3 , the omental and pelvic peritoneum<br />
being the most typical involved areas, and less commonly<br />
seen at different sites such as pleura 4 5 , pericardium 6 and tunica<br />
vaginalis 7-10 . Grossly, WDPMs are mostly solitary but can be<br />
multiple, and appear as gray to white, firm, papillary or nodular<br />
lesions generally measuring less than 2 cm in diameter, even if<br />
larger WDPMs (up to 6 cm) have been previously reported 1 2 .<br />
WDPM must be differentiated at one end of the spectrum from<br />
mesothelial hyperplastic proliferations and, at the other end,<br />
from malignant mesothelioma. In mesothelial hyperplasia, that<br />
not infrequently is characterized by a papillary architecture,<br />
the papillae have a very thin fibrous core if any, being in most<br />
cases composed exclusively of mesothelial cells organized in a<br />
pseudopapillary fashion. Moreover, a reactive flogistic process<br />
of moderate grade at least, is invariably seen in the adjacent serosa<br />
3 ; this is an uncommon finding in WDPMs. The differential<br />
diagnosis of malignant mesothelioma (MM) and WDPM can be,<br />
at times, very problematic, especially in bioptic material or in<br />
areas of malignant mesothelioma resembling WDPM. Thorough<br />
examination of the specimen, given that the material submitted<br />
for histological examination is representative of the entire<br />
lesion, should lead to the correct diagnosis in most instances.<br />
Their clinical and biological behavior is almost invariably benign<br />
and indolent, even though some have been reported as persistent,<br />
recurrent or even associated with an aggressive course<br />
or progression to MM 4 11 . The majority of such cases however<br />
might well represent undersampled malignant mesotheliomas<br />
from the beginning. In cases with poorer prognosis, overtreatment<br />
(adjuvant chemotherapy) may have been the main cause<br />
of morbidity and mortality associated with WDPMs 2 . It is very<br />
important to be aware of this pathologic entity, which occurs<br />
rarely and most commonly as an incidental finding. Accuracy<br />
and thorough examination is mandatory in order to exclude a<br />
malignant mesothelioma, which could manifest its invasivity<br />
and cytologic atypia only in focal areas. At the same time, it<br />
is necessary to be aware of the indolent biological behavior of<br />
WDPMs, when correctly diagnosed, in order to prevent overtreatment.




