ABSTRACTS from 16th International COnference on ... - CRRT Online
ABSTRACTS from 16th International COnference on ... - CRRT Online
ABSTRACTS from 16th International COnference on ... - CRRT Online

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<str<strong>on</strong>g>ABSTRACTS</str<strong>on</strong>g> FROM 17 TH INTERNATIONAL CONFERENCE ON <strong>CRRT</strong>,<br />
SAN DIEGO, FEB 14-17, 2012<br />
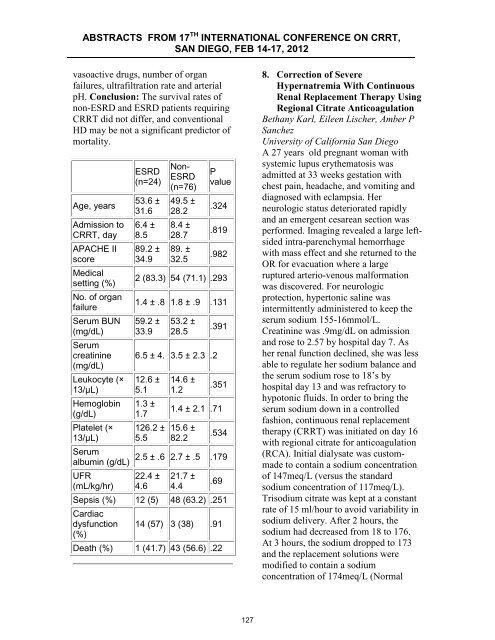
vasoactive drugs, number of organ<br />
failures, ultrafiltrati<strong>on</strong> rate and arterial<br />
pH. C<strong>on</strong>clusi<strong>on</strong>: The survival rates of<br />
n<strong>on</strong>-ESRD and ESRD patients requiring<br />
<strong>CRRT</strong> did not differ, and c<strong>on</strong>venti<strong>on</strong>al<br />
HD may be not a significant predictor of<br />
mortality.<br />
Age, years<br />
Admissi<strong>on</strong> to<br />
<strong>CRRT</strong>, day<br />
APACHE II<br />
score<br />
Medical<br />
setting (%)<br />
No. of organ<br />
failure<br />
Serum BUN<br />
(mg/dL)<br />
Serum<br />
creatinine<br />
(mg/dL)<br />
Leukocyte (×<br />
13/μL)<br />
Hemoglobin<br />
(g/dL)<br />
Platelet (×<br />
13/μL)<br />
Serum<br />
albumin (g/dL)<br />
UFR<br />
(mL/kg/hr)<br />
ESRD<br />
(n=24)<br />
53.6 ±<br />
31.6<br />
6.4 ±<br />
8.5<br />
89.2 ±<br />
34.9<br />
N<strong>on</strong>-<br />
ESRD<br />
(n=76)<br />
49.5 ±<br />
28.2<br />
8.4 ±<br />
28.7<br />
89. ±<br />
32.5<br />
P<br />
value<br />
.324<br />
.819<br />
.982<br />
2 (83.3) 54 (71.1) .293<br />
1.4 ± .8 1.8 ± .9 .131<br />
59.2 ±<br />
33.9<br />
53.2 ±<br />
28.5<br />
6.5 ± 4. 3.5 ± 2.3 .2<br />
12.6 ±<br />
5.1<br />
1.3 ±<br />
1.7<br />
126.2 ±<br />
5.5<br />
14.6 ±<br />
1.2<br />
.391<br />
.351<br />
1.4 ± 2.1 .71<br />
15.6 ±<br />
82.2<br />
.534<br />
2.5 ± .6 2.7 ± .5 .179<br />
22.4 ±<br />
4.6<br />
21.7 ±<br />
4.4<br />
.69<br />
Sepsis (%) 12 (5) 48 (63.2) .251<br />
Cardiac<br />
dysfuncti<strong>on</strong> 14 (57) 3 (38) .91<br />
(%)<br />
Death (%) 1 (41.7) 43 (56.6) .22<br />
8. Correcti<strong>on</strong> of Severe<br />
Hypernatremia With C<strong>on</strong>tinuous<br />
Renal Replacement Therapy Using<br />
Regi<strong>on</strong>al Citrate Anticoagulati<strong>on</strong><br />
Bethany Karl, Eileen Lischer, Amber P<br />
Sanchez<br />
University of California San Diego<br />
A 27 years old pregnant woman with<br />
systemic lupus erythematosis was<br />
admitted at 33 weeks gestati<strong>on</strong> with<br />
chest pain, headache, and vomiting and<br />
diagnosed with eclampsia. Her<br />
neurologic status deteriorated rapidly<br />
and an emergent cesarean secti<strong>on</strong> was<br />
performed. Imaging revealed a large leftsided<br />
intra-parenchymal hemorrhage<br />
with mass effect and she returned to the<br />
OR for evacuati<strong>on</strong> where a large<br />
ruptured arterio-venous malformati<strong>on</strong><br />
was discovered. For neurologic<br />
protecti<strong>on</strong>, hypert<strong>on</strong>ic saline was<br />
intermittently administered to keep the<br />
serum sodium 155-16mmol/L.<br />
Creatinine was .9mg/dL <strong>on</strong> admissi<strong>on</strong><br />
and rose to 2.57 by hospital day 7. As<br />
her renal functi<strong>on</strong> declined, she was less<br />
able to regulate her sodium balance and<br />
the serum sodium rose to 18’s by<br />
hospital day 13 and was refractory to<br />
hypot<strong>on</strong>ic fluids. In order to bring the<br />
serum sodium down in a c<strong>on</strong>trolled<br />
fashi<strong>on</strong>, c<strong>on</strong>tinuous renal replacement<br />
therapy (<strong>CRRT</strong>) was initiated <strong>on</strong> day 16<br />
with regi<strong>on</strong>al citrate for anticoagulati<strong>on</strong><br />
(RCA). Initial dialysate was custommade<br />
to c<strong>on</strong>tain a sodium c<strong>on</strong>centrati<strong>on</strong><br />
of 147meq/L (versus the standard<br />
sodium c<strong>on</strong>centrati<strong>on</strong> of 117meq/L).<br />
Trisodium citrate was kept at a c<strong>on</strong>stant<br />
rate of 15 ml/hour to avoid variability in<br />
sodium delivery. After 2 hours, the<br />
sodium had decreased <str<strong>on</strong>g>from</str<strong>on</strong>g> 18 to 176.<br />
At 3 hours, the sodium dropped to 173<br />
and the replacement soluti<strong>on</strong>s were<br />
modified to c<strong>on</strong>tain a sodium<br />
c<strong>on</strong>centrati<strong>on</strong> of 174meq/L (Normal<br />
127