ABSTRACTS from 16th International COnference on ... - CRRT Online
ABSTRACTS from 16th International COnference on ... - CRRT Online
ABSTRACTS from 16th International COnference on ... - CRRT Online

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>ABSTRACTS</str<strong>on</strong>g> FROM 17 TH INTERNATIONAL CONFERENCE ON <strong>CRRT</strong>,<br />
SAN DIEGO, FEB 14-17, 2012<br />
data of 89 ICU patients with AKI or<br />
acute-<strong>on</strong>-chr<strong>on</strong>ic kidney disease who<br />
received <strong>CRRT</strong>. We calculated the<br />
SAPS 3 and APACHE II score at the<br />
start of <strong>CRRT</strong>. Results: The average age<br />
of the 89 patients was 64.4±13.9 years.<br />
Fifty-nine (66.3%) patients were male.<br />
Eighteen (2.2%) patients had chr<strong>on</strong>ic<br />
kidney disease and thirty (33.7%)<br />
patients had diabetes. Sixty-two (69.8%)<br />
patients treated with mechanical<br />
ventilati<strong>on</strong>. The average systolic blood<br />
pressure was 85.9±27.4 mmHg, and<br />
sixty-four (71.9%) patients treated with<br />
vasopressor. The overall mortality was<br />
75.3%. The average SAPS 3 was<br />
89.4±14.9 and the average APACHE II<br />
score was 28.4±5.2. The SAPS 3 was<br />
higher in n<strong>on</strong>-survivors than survivors<br />
(p=.38). Sepsis was more comm<strong>on</strong> in<br />
n<strong>on</strong>-survivors than survivors (p=.36).<br />
There were no significant differences<br />
between the two groups for other<br />
c<strong>on</strong>diti<strong>on</strong>s. The variables influencing<br />
mortality <strong>on</strong> univariate analysis were<br />
SAPS 3 and presence of sepsis. The area<br />
under the receiver-operating<br />
characteristic curve for SAPS 3 was .69<br />
(95% CI. .54–.83). At a SAPS 3 of 84,<br />
the sensitivity for predicting mortality<br />
was 71.6% and the specificity was<br />
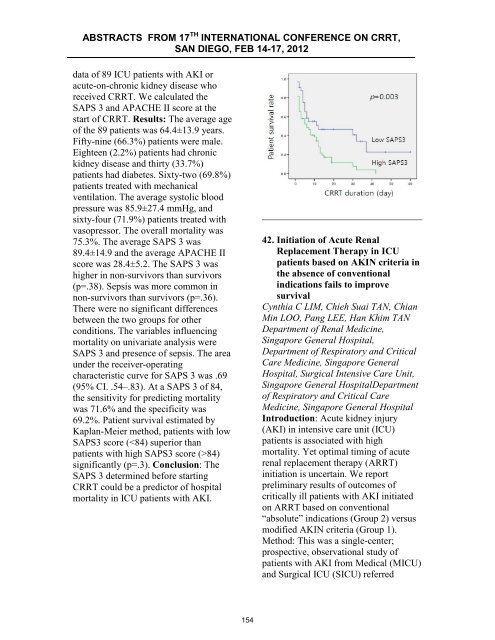
69.2%. Patient survival estimated by<br />
Kaplan-Meier method, patients with low<br />
SAPS3 score (84)<br />
significantly (p=.3). C<strong>on</strong>clusi<strong>on</strong>: The<br />
SAPS 3 determined before starting<br />
<strong>CRRT</strong> could be a predictor of hospital<br />
mortality in ICU patients with AKI.<br />
42. Initiati<strong>on</strong> of Acute Renal<br />
Replacement Therapy in ICU<br />
patients based <strong>on</strong> AKIN criteria in<br />
the absence of c<strong>on</strong>venti<strong>on</strong>al<br />
indicati<strong>on</strong>s fails to improve<br />
survival<br />
Cynthia C LIM, Chieh Suai TAN, Chian<br />
Min LOO, Pang LEE, Han Khim TAN<br />
Department of Renal Medicine,<br />
Singapore General Hospital,<br />
Department of Respiratory and Critical<br />
Care Medicine, Singapore General<br />
Hospital, Surgical Intensive Care Unit,<br />
Singapore General HospitalDepartment<br />
of Respiratory and Critical Care<br />
Medicine, Singapore General Hospital<br />
Introducti<strong>on</strong>: Acute kidney injury<br />
(AKI) in intensive care unit (ICU)<br />
patients is associated with high<br />
mortality. Yet optimal timing of acute<br />
renal replacement therapy (ARRT)<br />
initiati<strong>on</strong> is uncertain. We report<br />
preliminary results of outcomes of<br />
critically ill patients with AKI initiated<br />
<strong>on</strong> ARRT based <strong>on</strong> c<strong>on</strong>venti<strong>on</strong>al<br />
“absolute” indicati<strong>on</strong>s (Group 2) versus<br />
modified AKIN criteria (Group 1).<br />
Method: This was a single-center;<br />
prospective, observati<strong>on</strong>al study of<br />
patients with AKI <str<strong>on</strong>g>from</str<strong>on</strong>g> Medical (MICU)<br />
and Surgical ICU (SICU) referred<br />
154