Power to Prevent - National Diabetes Education Program - National ...
Power to Prevent - National Diabetes Education Program - National ...
Power to Prevent - National Diabetes Education Program - National ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
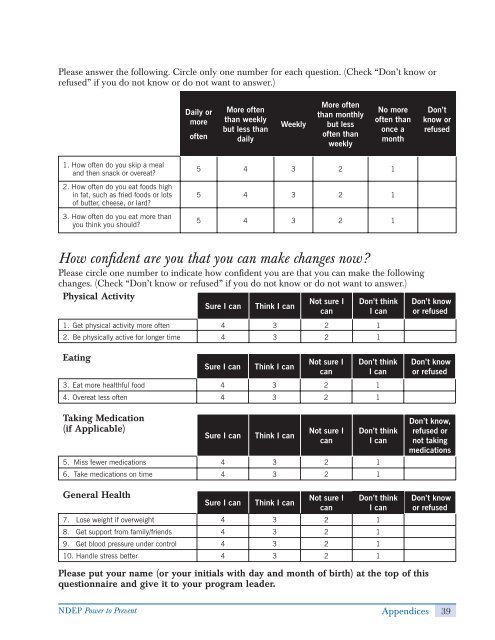
Please answer the following. Circle only one number for each question. (Check “Don’t know or<br />
refused” if you do not know or do not want <strong>to</strong> answer.)<br />
1. How<br />
often do you skip a meal<br />
and then snack or overeat?<br />
2. How<br />
often do you eat foods high<br />
in fat, such as fried foods or lots<br />
of butter, cheese, or lard?<br />
3. How<br />
often do you eat more than<br />
you think you should?<br />
General Health<br />
Daily or<br />
more<br />
often<br />
More often<br />
than weekly<br />
but less than<br />
daily<br />
Weekly<br />
Sure I can Think I can<br />
More often<br />
than monthly<br />
but less<br />
often than<br />
weekly<br />
Not sure I<br />
can<br />
Don’t think<br />
I can<br />
7. Lose weight if overweight 4 3 2 1<br />
8. Get support from family/friends 4 3 2 1<br />
9. Get blood pressure under control 4 3 2 1<br />
10. Handle stress better 4 3 2 1<br />
No more<br />
often than<br />
once a<br />
month<br />
5 4 3 2 1<br />
5 4 3 2 1<br />
5 4 3 2 1<br />
How confdent are you that you can make changes now?<br />
Please circle one number <strong>to</strong> indicate how confdent you are that you can make the following<br />
changes. (Check “Don’t know or refused” if you do not know or do not want <strong>to</strong> answer.)<br />
Physical Activity<br />
Sure I can Think I can<br />
Not sure I<br />
can<br />
Don’t think<br />
I can<br />
1. Get physical activity more often 4 3 2 1<br />
2. Be physically active for longer time 4 3 2 1<br />
Eating<br />
Sure I can Think I can<br />
Not sure I<br />
can<br />
Don’t think<br />
I can<br />
3. Eat more healthful food 4 3 2 1<br />
4. Overeat less often 4 3 2 1<br />
Taking Medication<br />
(if Applicable)<br />
Sure I can Think I can<br />
Not sure I<br />
can<br />
Don’t think<br />
I can<br />
5. Miss fewer medications 4 3 2 1<br />
6. Take medications on time 4 3 2 1<br />
Please put your name (or your initials with day and month of birth) at the <strong>to</strong>p of this<br />
questionnaire and give it <strong>to</strong> your program leader.<br />
Don’t<br />
know or<br />
refused<br />
Don’t know<br />
or refused<br />
Don’t know<br />
or refused<br />
Don’t know,<br />
refused or<br />
not taking<br />
medications<br />
Don’t know<br />
or refused<br />
NDEP <strong>Power</strong> <strong>to</strong> <strong>Prevent</strong> Appendices 39