6th European Conference - Academic Conferences
6th European Conference - Academic Conferences
6th European Conference - Academic Conferences

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Shada Alsalamah et al.<br />
control over shared patient medical information in the future. This would be hard to achieve without<br />
the identification of the IS issues and emerging needs in this dynamic environment through the study<br />
of a real-life scenario.<br />
6. Conclusion<br />
There is a shift today towards collaboration among different healthcare organisations for a common<br />
goal of better patient treatment through moving to a patient centric control. In achieving this, an IS is<br />
essential to the effectiveness, dynamism, and potential of collaborative working if the full potential is<br />
to be realised. The provision of an SCE for multiple organisations has proved to be a challenge. This<br />
paper presents the results of a study into the inter-professional communication needs of a secure<br />
cross organisation’s information-sharing system in the healthcare domain. The findings in this paper<br />
provide the initial results from the first stage of the project and they will be used to inform further<br />
investigation in the ensuing stages to identify the key IS issues affecting inter-professional<br />
communication, as well as the IS needs in this environment which facilitate the sharing of information<br />
throughout the distributed domain.<br />
7. Appendix A<br />
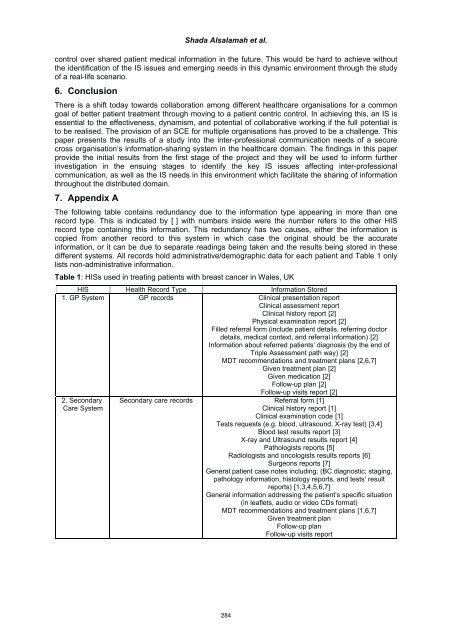
The following table contains redundancy due to the information type appearing in more than one<br />
record type. This is indicated by [-] with numbers inside were the number refers to the other HIS<br />
record type containing this information. This redundancy has two causes, either the information is<br />
copied from another record to this system in which case the original should be the accurate<br />
information, or it can be due to separate readings being taken and the results being stored in these<br />
different systems. All records hold administrative/demographic data for each patient and Table 1 only<br />
lists non-administrative information.<br />
Table 1: HISs used in treating patients with breast cancer in Wales, UK<br />
HIS Health Record Type Information Stored<br />
1. GP-System GP-records Clinical presentation report<br />
Clinical assessment report<br />
Clinical history report-[2]<br />
Physical examination report-[2]<br />
Filled referral form (include patient details, referring doctor<br />
details, medical context, and referral information)-[2]<br />
Information about referred patients’ diagnosis (by the end of<br />
Triple Assessment path way)-[2]<br />
MDT recommendations and treatment plans-[2,6,7]<br />
Given treatment plan-[2]<br />
Given medication-[2]<br />
Follow-up plan-[2]<br />
2. Secondary-<br />
Care-System<br />
Follow-up visits report-[2]<br />
Secondary-care-records Referral form-[1]<br />
Clinical history report-[1]<br />
Clinical examination code-[1]<br />
Tests requests (e.g. blood, ultrasound, X-ray test)-[3,4]<br />
Blood test results report-[3]<br />
X-ray and Ultrasound results report-[4]<br />
Pathologists reports-[5]<br />
Radiologists and oncologists results reports-[6]<br />
Surgeons reports-[7]<br />
General patient case notes including: (BC diagnostic, staging,<br />
pathology information, histology reports, and tests’ result<br />
reports)-[1,3,4,5,6,7]<br />
General information addressing the patient’s specific situation<br />
(in leaflets, audio or video CDs format)<br />
MDT recommendations and treatment plans-[1,6,7]<br />
Given treatment plan<br />
Follow-up plan<br />
Follow-up visits report<br />
284