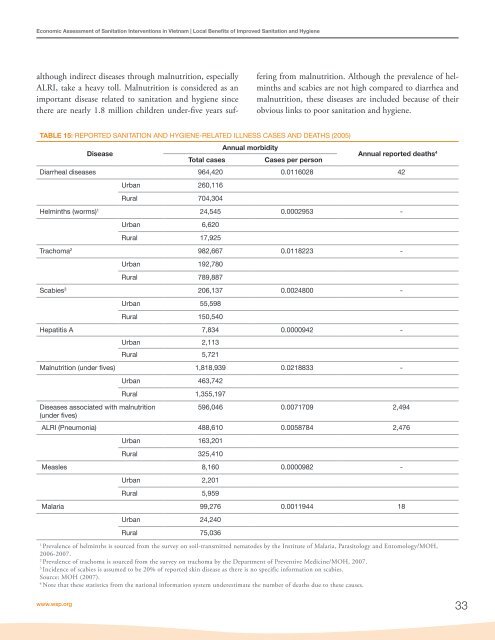
IV.Local Benefits <strong>of</strong> Improved <strong>Sanitation</strong>and Hygiene32This chapter discusses the follow<strong>in</strong>g local impacts <strong>of</strong> improvedsanitation and hygiene:• Health (section 4.1)• Water (section 4.2)• Access time (section 4.3)• Intangibles (section 4.4)• External environment (section 4.5)• Reuse (section 4.6)• Summary <strong>of</strong> local benefits (section 4.7)4.1 HEALTHOne <strong>of</strong> the major arguments commonly used <strong>in</strong> favor <strong>of</strong>improv<strong>in</strong>g sanitation is a reduction <strong>in</strong> disease <strong>in</strong>cidence,and the various associated health-related benefits. There aremany diseases associated with poor sanitation and hygienepractices, <strong>in</strong>clud<strong>in</strong>g diarrhea, dysentery, cholera, salmonellosis,shigellosis, typhoid fever, hepatitis A, trachoma, andsome parasitic diseases (ascariasis, trichuriasis, hookworm,schistosomiasis) (see Annex Table A6). Disease and povertyare l<strong>in</strong>ked <strong>in</strong> a vicious circle, and hence disease reductioncan lift populations out <strong>of</strong> poverty, or prevent them fromfall<strong>in</strong>g <strong>in</strong>to poverty. Less disease means less treatment seek<strong>in</strong>gcosts and a ga<strong>in</strong> <strong>in</strong> healthy time, lead<strong>in</strong>g to more timefor productive or leisure activities, which have a direct welfareimpact. When productive time ga<strong>in</strong>ed leads to a net<strong>in</strong>crease <strong>in</strong> economic activity, it can contribute to economicgrowth and poverty reduction. Disease reduction also leadsto sav<strong>in</strong>gs for society, such as health care and other statebenefits for chronic sufferers.ESI study, phase 1 (<strong>WSP</strong>, 2009) reported the estimatedcases and deaths per year from selected diseases attributedto poor sanitation <strong>in</strong> <strong>Vietnam</strong>. It showed that, <strong>of</strong> the diseaseattributed to poor sanitation, diarrhea has the highestnumber <strong>of</strong> cases at 7.05 million per year. Diarrhea is alsothe ma<strong>in</strong> cause <strong>of</strong> death from poor sanitation and hygiene,account<strong>in</strong>g for around 4,600 deaths per year <strong>in</strong> <strong>Vietnam</strong>.Malnutrition-related diseases, <strong>in</strong> particular acute lowerrespiratory <strong>in</strong>fection (ALRI), account for an estimated1,500 deaths per year attributed to poor sanitation, followedby malaria with 600 deaths per year. In 2004, theWorld Health Organization estimated that diarrheal diseaseaccounted for 12% <strong>of</strong> overall deaths <strong>of</strong> 0-14 year olds <strong>in</strong><strong>Vietnam</strong>, and 50% <strong>of</strong> <strong>in</strong>fectious and parasitic diseases. Thenumber <strong>of</strong> deaths from diarrhea exceeded the number <strong>of</strong>deaths from <strong>in</strong>tentional and un<strong>in</strong>tentional <strong>in</strong>juries, <strong>in</strong>clud<strong>in</strong>groad traffic accidents.Diseases such as scabies, helm<strong>in</strong>ths and hepatitis A appearto account for only a small proportion <strong>of</strong> the total diseaseburden. There are no reported cases <strong>in</strong> <strong>of</strong>ficial statistics <strong>of</strong>mortality from these diseases. Collectively, they account foronly about 5.4% <strong>of</strong> the number <strong>of</strong> cases. However, theircollective <strong>in</strong>fluence on the quality <strong>of</strong> life cannot be ignored.The prevalence <strong>of</strong> trachoma is still high as it is endemic <strong>in</strong><strong>Vietnam</strong>. Treatment is sought for only a small fraction <strong>of</strong>cases, so healthcare costs would be much higher if all suffererssought formal health care for every <strong>in</strong>cidence <strong>of</strong> disease.4.1.1 DISEASE BURDEN OF POOR SANITATIONAND HYGIENETable 15 presents the data available from the national health<strong>in</strong>formation system <strong>in</strong> <strong>Vietnam</strong> on the number <strong>of</strong> cases anddeaths result<strong>in</strong>g from key sanitation and hygiene-relateddiseases. Although these data are not representative <strong>of</strong> thetotal disease burden at national level due to underreport<strong>in</strong>g,they do provide an <strong>in</strong>dication <strong>of</strong> which diseases are <strong>of</strong> mostsignificance nationally, and aid the selection <strong>of</strong> diseases to<strong>in</strong>clude <strong>in</strong> this present study.Table 15 shows that there were 964,420 cases <strong>of</strong> diarrhealdiseases <strong>in</strong> 2005. The actual number <strong>of</strong> cases is expectedto be many times higher, as concluded <strong>in</strong> the ESI phase 1study (<strong>WSP</strong>, 2009). Diarrhea is also reported as the majordirect cause <strong>of</strong> death due to poor sanitation and hygiene,<strong>Economic</strong> <strong>Assessment</strong> <strong>of</strong> <strong>Sanitation</strong> <strong>Interventions</strong>
<strong>Economic</strong> <strong>Assessment</strong> <strong>of</strong> <strong>Sanitation</strong> <strong>Interventions</strong> <strong>in</strong> <strong>Vietnam</strong> | Local Benefits <strong>of</strong> Improved <strong>Sanitation</strong> and Hygienealthough <strong>in</strong>direct diseases through malnutrition, especiallyALRI, take a heavy toll. Malnutrition is considered as animportant disease related to sanitation and hygiene s<strong>in</strong>cethere are nearly 1.8 million children under-five years suffer<strong>in</strong>gfrom malnutrition. Although the prevalence <strong>of</strong> helm<strong>in</strong>thsand scabies are not high compared to diarrhea andmalnutrition, these diseases are <strong>in</strong>cluded because <strong>of</strong> theirobvious l<strong>in</strong>ks to poor sanitation and hygiene.TABLE 15: REPORTED SANITATION AND HYGIENE-RELATED ILLNESS CASES AND DEATHS (2005)DiseaseTotal casesAnnual morbidityCases per personAnnual reported deaths 4Diarrheal diseases 964,420 0.0116028 42Urban 260,116Rural 704,304Helm<strong>in</strong>ths (worms) 1 24,545 0.0002953 -Urban 6,620Rural 17,925Trachoma 2 982,667 0.0118223 -Urban 192,780Rural 789,887Scabies 3 206,137 0.0024800 -Urban 55,598Rural 150,540Hepatitis A 7,834 0.0000942 -Urban 2,113Rural 5,721Malnutrition (under fives) 1,818,939 0.0218833 -Diseases associated with malnutrition(under fives)Urban 463,742Rural 1,355,197596,046 0.0071709 2,494ALRI (Pneumonia) 488,610 0.0058784 2,476Urban 163,201Rural 325,410Measles 8,160 0.0000982 -Urban 2,201Rural 5,959Malaria 99,276 0.0011944 18Urban 24,240Rural 75,0361Prevalence <strong>of</strong> helm<strong>in</strong>ths is sourced from the survey on soil-transmitted nematodes by the Institute <strong>of</strong> Malaria, Parasitology and Entomology/MOH,2006-2007.2Prevalence <strong>of</strong> trachoma is sourced from the survey on trachoma by the Department <strong>of</strong> Preventive Medic<strong>in</strong>e/MOH, 2007.3Incidence <strong>of</strong> scabies is assumed to be 20% <strong>of</strong> reported sk<strong>in</strong> disease as there is no specific <strong>in</strong>formation on scabies.Source: MOH (2007).4Note that these statistics from the national <strong>in</strong>formation system underestimate the number <strong>of</strong> deaths due to these causes.www.wsp.org33