

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
A<br />
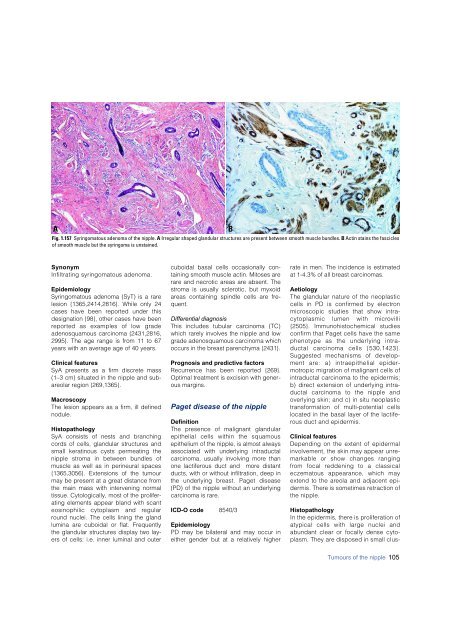
Fig. 1.157 Syringomatous adenoma of the nipple. A Irregular shaped glandular structures are present between smooth muscle bundles. B Actin stains the fascicles<br />
of smooth muscle but the syringoma is unstained.<br />
B<br />
S y n o n y m<br />
Infiltrating syringomatous adenoma.<br />
Epidemiology<br />
Syringomatous adenoma (SyT) is a rare<br />
lesion {1365,2414,2816}. While only 24<br />
cases have been reported under this<br />
designation {98}, other cases have been<br />
re p o rted as examples of low grade<br />
adenosquamous <strong>carcinoma</strong> {2431,2816,<br />
2995}. The age range is from 11 to 67<br />
years with an average age of 40 years.<br />
Clinical features<br />
SyA presents as a firm discrete mass<br />
(1–3 cm) situated in the nipple and subareolar<br />
region {269,1365}.<br />
Macroscopy<br />
The lesion appears as a firm, ill defined<br />
nodule.<br />
Histopathology<br />
SyA consists of nests and branching<br />
cords of cells, glandular structures and<br />
small keratinous cysts permeating the<br />
nipple stroma in between bundles of<br />
muscle as well as in perineural spaces<br />
{1365,3056}. Extensions of the tumour<br />
may be present at a great distance from<br />
the main mass with intervening normal<br />
tissue. Cytologically, most of the proliferating<br />
elements appear bland with scant<br />
eosinophilic cytoplasm and re g u l a r<br />
round nuclei. The cells lining the gland<br />
lumina are cuboidal or flat. Frequently<br />
the glandular structures display two layers<br />
of cells: i.e. inner luminal and outer<br />
cuboidal basal cells occasionally containing<br />
smooth muscle actin. Mitoses are<br />
rare and necrotic areas are absent. The<br />
stroma is usually sclerotic, but myxoid<br />
areas containing spindle cells are frequent.<br />
Differential diagnosis<br />
This includes tubular <strong>carcinoma</strong> (TC)<br />
which rarely involves the nipple and low<br />
grade adenosquamous <strong>carcinoma</strong> which<br />
occurs in the <strong>breast</strong> parenchyma {2431}.<br />
Prognosis and predictive factors<br />
Recurrence has been reported {269}.<br />
Optimal treatment is excision with generous<br />
margins.<br />
Paget disease of the nipple<br />
Definition<br />
The presence of malignant glandular<br />
epithelial cells within the squamous<br />
epithelium of the nipple, is almost always<br />
associated with underlying intraductal<br />
<strong>carcinoma</strong>, usually involving more than<br />
one lactiferous duct and more distant<br />
ducts, with or without infiltration, deep in<br />
the underlying <strong>breast</strong>. Paget disease<br />
(PD) of the nipple without an underlying<br />
<strong>carcinoma</strong> is rare.<br />
ICD-O code 8540/3<br />
Epidemiology<br />
PD may be bilateral and may occur in<br />
either gender but at a relatively higher<br />
rate in men. The incidence is estimated<br />
at 1-4.3% of all <strong>breast</strong> <strong>carcinoma</strong>s.<br />
Aetiology<br />
The glandular nature of the neoplastic<br />
cells in PD is confirmed by electro n<br />
m i c roscopic studies that show intracytoplasmic<br />
lumen with micro v i l l i<br />
{ 2 5 05}. Immunohistochemical studies<br />
c o n f i rm that Paget cells have the same<br />
phenotype as the underlying intraductal<br />
<strong>carcinoma</strong> cells {530,1423}.<br />
Suggested mechanisms of development<br />
are: a) intraepithelial e p i d e r-<br />
m o t ropic migration of malignant cells of<br />
intraductal <strong>carcinoma</strong> to the epiderm i s ;<br />
b) direct extension of underlying intraductal<br />
<strong>carcinoma</strong> to the nipple and<br />
overlying skin; and c) in situ neoplastic<br />
t r a n s f o rmation of multi-potential cells<br />
located in the basal layer of the lactiferous<br />
duct and epiderm i s .<br />
Clinical features<br />
Depending on the extent of epiderm a l<br />
involvement, the skin may appear unremarkable<br />
or show changes ranging<br />
f rom focal reddening to a classical<br />
eczematous appearance, which may<br />
extend to the areola and adjacent epid<br />
e rmis. There is sometimes retraction of<br />
the nipple.<br />
Histopathology<br />
In the epidermis, there is proliferation of<br />
atypical cells with large nuclei and<br />
abundant clear or focally dense cytoplasm.<br />
They are disposed in small clus-<br />
Tumours of the nipple 105













