

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Prognosis and predictive factors<br />
The clinical course of uterine carcinosarcoma<br />
is generally aggressive with a poor<br />
overall prognosis, considerably worse<br />
than that of a poorly diff e re n t i a t e d<br />
endometrial <strong>carcinoma</strong>. The pattern of<br />
spread is generally similar to that of high<br />
grade endometrial <strong>carcinoma</strong>, and deep<br />
myometrial invasion and extrauterine<br />
spread are often observed at the time of<br />
presentation. The clinical staging is the<br />
same as that for endometrial <strong>carcinoma</strong>.<br />
Some studies have found no independent<br />
prognostic factors other than tumour<br />
stage, whereas others have found that<br />
the characteristics of the epithelial component<br />
such as high grade <strong>carcinoma</strong>,<br />
including serous or clear cell components,<br />
are associated with a worse prognosis<br />
{2692}. Previously, it was thought<br />
that the presence of heterologous mesenchymal<br />
components indicated a worse<br />
outcome; however, recent larger studies<br />
have suggested that the histological features<br />
of the mesenchymal component<br />
bear no relationship to the overall prognosis<br />
{2692}.<br />
The biological behaviour of uterine carcinosarcomas<br />
is more akin to high grade<br />
endometrial <strong>carcinoma</strong>s than to uterine<br />
sarcomas {282,2692}. Carcinosarcomas<br />
primarily spread via lymphatics, whereas<br />
pure uterine sarcomas commonly spread<br />
h a e m a t o g e n o u s l y. Detailed studies of<br />
uterine carcinosarcoma have shown that<br />
metastatic foci and foci within lymphatic<br />
or vascular spaces are commonly <strong>carcinoma</strong>tous<br />
with pure sarcomatous elements<br />
being rare {282,2692,2767}.<br />
Although the tumour stage is the most<br />
important prognostic factor, recurrences<br />
may be encountered even in those rare<br />
cases lacking myometrial infiltration.<br />
However, tumours confined to an otherwise<br />
benign polyp appear to have a<br />
somewhat better outcome {188,1382}.<br />
Adenosarcoma<br />
Definition<br />
Adenosarcoma is a biphasic neoplasm<br />
containing a benign epithelial component<br />
and a sarcomatous mesenchymal<br />
component.<br />
Epidemiology<br />
Adenosarcoma occurs in women of all<br />
ages, ranging from 15-90 years with a<br />
median age at diagnosis of 58.<br />
Adenosarcomas have been reported in<br />
women undergoing tamoxifen therapy for<br />
<strong>breast</strong> cancer {509} and occasionally<br />
after prior pelvic radiation {515}. There is<br />
no association of adenosarcoma with<br />
obesity or hypertension.<br />
Clinical features<br />
Typical symptoms of patients with<br />
a d e n o s a rcoma are abnormal vaginal<br />
bleeding, an enlarged uterus and tissue<br />
p rotruding from the external os. The<br />
tumour may not be correctly diagnosed<br />
as adenosarcoma until re-excision of a<br />
recurrent polypoid lesion {515}.<br />
Macroscopy<br />
Adenosarcomas typically grow as exophytic<br />
polypoid masses that extend into<br />
the uterine cavity. Rarely, they may arise<br />
in the myometrium, presumably fro m<br />
adenomyosis. Although the tumour is<br />
usually a single polypoid mass, it sometimes<br />
may present as multiple papillary<br />
masses. On sectioning, the surface is tan<br />
b rown with foci of haemorrhage and<br />
necrosis. Small cysts are frequently present.<br />
Most adenosarcomas do not invade<br />
the myometrium.<br />
Histopathology<br />
Under low magnification a leaf-like pattern<br />
closely resembling phyllodes tumour of<br />
the <strong>breast</strong> is observed. Isolated glands,<br />
often dilated and compressed into thin<br />
slits, are dispersed throughout the mesenchymal<br />
component. Characte- ristically,<br />
t h e re is stromal condensation surro u n d i n g<br />
the glands and clefts. It is in these are a s<br />
w h e re the greatest degree of stro m a l<br />
atypia and mitotic activity is present. By<br />
definition the epithelium is benign and<br />
may show focal metaplastic changes. The<br />
mesenchymal component of an<br />
a d e n o s a rcoma is generally a low grade<br />
homologous stromal sarcoma containing<br />
v a rying amounts of fibrous tissue and<br />
smooth muscle. Mesenchymal mitotic figu<br />
res, usually stated to be more than one<br />
per 10 high power fields, are re q u i red in<br />
the hypercellular cuffs. Cytological atypia<br />
is typically only mild, but is occasionally<br />
moderate. Sex cord-like components<br />
resembling those in endometrial stro m a l<br />
s a rcomas are found in less than 10% of<br />
a d e n o s a rcomas. Heterologous components<br />
consisting of striated muscle (most<br />
commonly), cartilage, fat and other components<br />
are present in approximately 10-<br />
15% of tumours The diagnosis of sarc o-<br />
matous overgrowth is made if the pure<br />
A<br />
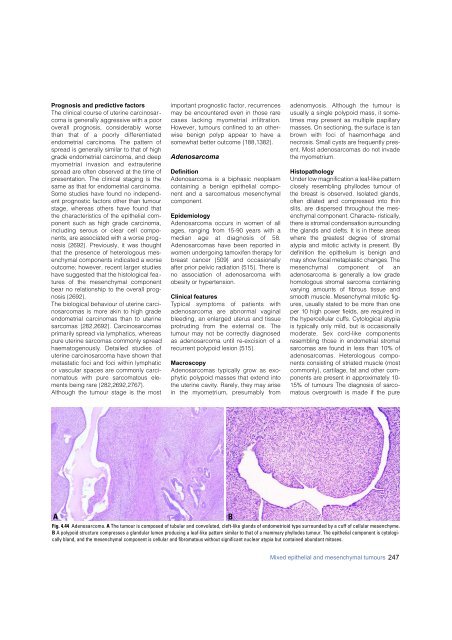
Fig. 4.44 Adenosarcoma. A The tumour is composed of tubular and convoluted, cleft-like glands of endometrioid type surrounded by a cuff of cellular mesenchyme.<br />
B A polypoid structure compresses a glandular lumen producing a leaf-like pattern similar to that of a mammary phyllodes tumour. The epithelial component is cytologically<br />
bland, and the mesenchymal component is cellular and fibromatous without significant nuclear atypia but contained abundant mitoses.<br />
B<br />
Mixed epithelial and mesenchymal tumours 247













