

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
evidence of neuroendocrine diff e re n t i a-<br />
tion {2533}. These proteins are identifiable<br />
by immunohistochemical and<br />
immunoblot analysis. Poorly and moderately<br />
diff e rentiated endocrine bre a s t<br />
c a rcinomas of the alveolar subtype, in<br />
general, express chromogranin A. The<br />
mRNA specific for chromogranin A is<br />
detectable by in situ hybridization technique<br />
{2535}. About 50% of well or<br />
moderately diff e rentiated tumours<br />
e x p ress chromogranin B and A and<br />
only 16% express synaptophysin<br />
{2535}. A monoclonal antibody against<br />
n e u rone-specific enolase (NSE) has<br />
also been used and is expressed in<br />
100% of small cell <strong>carcinoma</strong>s of the<br />
b reast {2662}, whereas chromogranin A<br />
and synaptophysin are expressed in<br />
about 50% of such cases. In addition,<br />
20% of small cell mammary carc i n o m a s<br />
e x p ress thyroid transcription factor- 1<br />
(TTF-1) {2661}.<br />
Immunodetection of pan-endocrine<br />
markers may fail to recognize endocrine<br />
tumours, which produce but do<br />
not retain the specific antigen in the<br />
cells. Estrogen (ER) and pro g e s t e ro n e<br />
receptors (PR) are expressed in the<br />
majority of tumour cells in well diff e re n-<br />
tiated tumours {2535}, and in more than<br />
50% of small cell <strong>carcinoma</strong>s {2662}.<br />
E x p ression of somatostatin re c e p t o r s<br />
(SSR), a known feature of tumours<br />
showing neuroendocrine diff e re n t i a t i o n ,<br />
has been demonstrated in endocrine<br />
b reast <strong>carcinoma</strong>s as well {2169}.<br />
U l t r a s t r u c t u r e<br />
D i ff e rent types of dense core granules,<br />
whose neuro s e c re t o ry nature is conf<br />
i rmed by ultrastructural immunolocalization<br />
of chromogranin A have been<br />
identified by electron microscopy in<br />
endocrine <strong>breast</strong> <strong>carcinoma</strong>s {397}.<br />
The presence of clear vesicles of presynaptic<br />
type is correlated with the<br />
e x p ression of synaptophysin.<br />
Both dense core granules and mucin<br />
vacuoles are present in neuro e n d o c r i n e<br />
mucinous <strong>carcinoma</strong>s {1265}.<br />
G e n e t i c s<br />
N e u roendocrine <strong>breast</strong> carc i n o m a s<br />
have not been correlated to specific<br />
gene mutations.<br />
Postulated normal counterpart<br />
A r g y rophilic and chromogranin A-re a c-<br />
tive cells, located between the basal<br />
myoepithelial and the luminal epithelial<br />
cells, have been demonstrated in histologically<br />
normal <strong>breast</strong> tissue surro u n d-<br />
ing infiltrating and in situ neuro e n-<br />
docrine <strong>breast</strong> <strong>carcinoma</strong>s {382,1995,<br />
2 5 4 2 , 2 9 5 6 } .<br />
Prognosis and predictive factors<br />
Histological grading is one of the most<br />
i m p o rtant prognostic parameters.<br />
NE <strong>breast</strong> <strong>carcinoma</strong>s may be graded<br />
using classical criteria described elsew<br />
h e re .<br />
Excluding the rare small cell variety,<br />
45% of NE <strong>breast</strong> <strong>carcinoma</strong>s are well<br />
d i ff e rentiated, 40% are moderately diff<br />
e rentiated, and only 15% are poorly diff<br />
e rentiated. Small cell NE carc i n o m a s<br />
should be considered as undiff e re n t i a t-<br />
ed <strong>carcinoma</strong>s {2535}.<br />
Mucinous diff e rentiation is a favourable<br />
p rognostic factor {2535}.<br />
The prognosis of primary small cell <strong>carcinoma</strong>s<br />
of the <strong>breast</strong> depends on the<br />
stage of disease at the time of diagnosis.<br />
It has been demonstrated that low<br />
stage small cell <strong>carcinoma</strong>s respond to<br />
conventional treatment without pro g re s-<br />
sion of the disease at a follow up of 33<br />
to 48 months {2662}.<br />
<strong>Invasive</strong> papillary <strong>carcinoma</strong><br />
Definition<br />
When papillary intraductal carc i n o m a s<br />
invade, they generally assume the patt<br />
e rn of infiltrating duct <strong>carcinoma</strong> and<br />
lack a papillary arc h i t e c t u re. Most of the<br />
published literature concerning papillary<br />
c a rcinomas of the <strong>breast</strong> probably include<br />
both invasive and in situ papillary<br />
lesions as they do not generally specify<br />
f e a t u res of an invasive process {413,<br />
603,969,1269,1604,1618,1834}. In this<br />
section, however, only data concern i n g<br />
invasive papillary <strong>carcinoma</strong>s will be<br />
reviewed. <strong>Invasive</strong> papillary carc i n o m a s<br />
comprise less than 1-2% of invasive<br />
b reast cancers, and are characterized by<br />
a relatively good prognosis {879,2567}.<br />
ICD-O code 8503/3<br />
Clinical features<br />
<strong>Invasive</strong> papillary <strong>carcinoma</strong>s are diagnosed<br />
predominantly in postmenopausal<br />
patients. Fisher et al. {879} noted a disproportionate<br />
number of cases in non-<br />
Caucasian women. Similar to medullary<br />
<strong>carcinoma</strong>s, Fisher et al. noted that a<br />
significant pro p o rtion of patients with<br />
invasive papillary <strong>carcinoma</strong> exhibit axill<br />
a ry lymphadenopathy suggestive of<br />
metastatic disease, but which on pathological<br />
examination is due to benign<br />
reactive changes {879}.<br />
M a m m o g r a p h i c a l l y, invasive papillary<br />
c a rcinoma is usually characterized by<br />
nodular densities which may be multiple,<br />
and are frequently lobulated {1880, 2567}.<br />
These lesions are often hypoechoic on<br />
ultrasound {1827}. One study noted the<br />
d i fficulty in distinguishing between intracystic<br />
papillary <strong>carcinoma</strong>, intracystic<br />
p a p i l l a ry <strong>carcinoma</strong> with invasion, and<br />
invasive papillary <strong>carcinoma</strong> {1827}.<br />
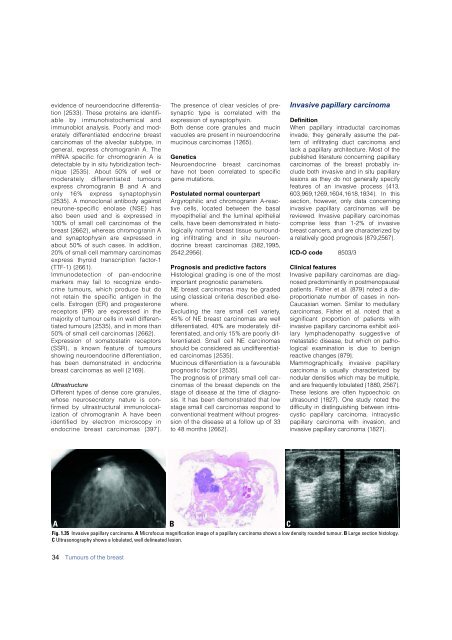
A<br />
B<br />
Fig. 1.35 <strong>Invasive</strong> papillary <strong>carcinoma</strong>. A Microfocus magnification image of a papillary <strong>carcinoma</strong> shows a low density rounded tumour. B Large section histology.<br />
C Ultrasonography shows a lobulated, well delineated lesion.<br />
C<br />
34 Tumours of the <strong>breast</strong>













