

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Benign epithelial proliferations<br />
G. Bussolati<br />
F.A. Tavassoli<br />
B.B. Nielsen<br />
I.O. Ellis<br />
G. MacGrogan<br />
L o c a l i z a t i o n<br />
T h e re is little data on location or laterality<br />
of most benign <strong>breast</strong> lesions. As<br />
with <strong>carcinoma</strong>, the majority arise within<br />
the terminal duct lobular unit (TDLU). A<br />
major exception is the benign solitary<br />
intraductal papilloma, appro x i m a t e l y<br />
90% of which occurs in the large ducts<br />
in the central region of the bre a s t<br />
{1098}. Other benign lesions specific to<br />
the nipple areolar complex include nipple<br />
adenoma and syringoma and are<br />
discussed in the chapter on nipple.<br />
Clinical features<br />
The predominant presenting symptoms<br />
in women attending a <strong>breast</strong> clinic are<br />
described in the section on <strong>Invasive</strong><br />
C a rcinoma, where signs and symptoms<br />
most likely to be associated with a low<br />
risk of malignancy are described. The<br />
f requency of benign conditions varies<br />
considerably with the age of the patient.<br />
F i b roadenoma is most frequent in<br />
younger patients, other localized benign<br />
lesions and cysts occur most fre q u e n t l y<br />
in women between the ages of 30 and<br />
50. This contrasts with carc i n o m a ,<br />
which is rare below the age of 40.<br />
The mammographic appearances of<br />
benign epithelial lesions are varied but<br />
common lesions such as cysts are typically<br />
seen as well defined or lobulated<br />
mass lesions. Calcification is also a<br />
common feature of fibrocystic change<br />
and sclerosing adenosis. Other benign<br />
lesions such as radial scar, complex<br />
s c l e rosing lesion and fat necrosis can<br />
p roduce ill defined or spiculate mass<br />
lesions, which are indistinguishable<br />
f rom some forms of <strong>breast</strong> carc i n o m a .<br />
A d e n o s i s<br />
D e f i n i t i o n<br />
A frequent, benign, proliferative pro c e s s<br />
that affects mainly the lobular (acinar)<br />
component of the <strong>breast</strong> parenchyma.<br />
It can be accompanied by fibro s i s<br />
causing considerable distortion of the<br />
glands simulating an invasive pro c e s s .<br />
F requently it is a small and micro s c o p i c<br />
change, but it may be widespread. In<br />
some instances, it may form a palpable<br />
mass and has been called nodular<br />
adenosis or adenosis tumour. Several<br />
histological types have been described,<br />
but there is not complete agreement on<br />
their designation. Only the most fre q u e n t<br />
variants are discussed.<br />
Radial scar/complex sclerosing lesion<br />
which incorporates a combination of<br />
benign changes including adenosis is<br />
also included in this section.<br />
E p i d e m i o l o g y<br />
This lesion occurs most frequently in<br />
women in their third and fourth decade.<br />
Macroscopy<br />
Adenosis may be non-distinctive, showing<br />
unremarkable fibrous or cystic<br />
b reast tissue. A few cases assume the<br />
appearance of a firm rubbery gre y<br />
mass.<br />
Histopathology<br />
Adenosis in its simplest form is characterized<br />
by a usually loosely structure d<br />
p roliferation of acinar or tubular struct<br />
u res, composed of an epithelial and<br />
myoepithelial cell layer and surro u n d e d<br />
by a basement membrane.<br />
Sclerosing adenosis<br />
S c l e rosing adenosis (SA) is characterized<br />
by a compact proliferation of acini<br />
with preservation of the luminal epithelial<br />
and the peripheral myoepithelial<br />
(ME) cell layers along with a surro u n d-<br />
ing basement membrane. These elements<br />
can easily be demonstrated by<br />
immunohistochemical staining for keratin,<br />
smooth-muscle actin and laminin,<br />
re s p e c t i v e l y. Although compression or<br />
attenuation of the acini by surro u n d i n g<br />
f i b rosis may be marked, sclero s i n g<br />
adenosis nearly always retains an<br />
organic or lobulated configuration often<br />
best observed at low power view.<br />
M i c rocalcifications are common within<br />
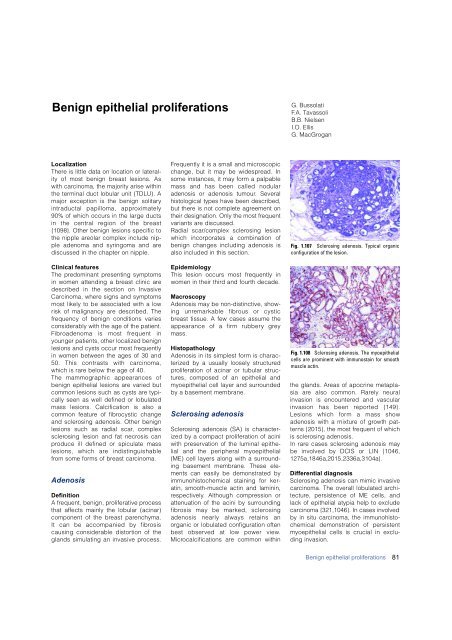
Fig. 1.107 Sclerosing adenosis. Typical organic<br />
configuration of the lesion.<br />
Fig. 1.108 Sclerosing adenosis. The myoepithelial<br />
cells are prominent with immunostain for smooth<br />
muscle actin.<br />
the glands. Areas of apocrine metaplasia<br />
are also common. Rarely neural<br />
invasion is encountered and vascular<br />
invasion has been re p o rted {149}.<br />
Lesions which form a mass show<br />
adenosis with a mixture of growth patt<br />
e rns {2015}, the most frequent of which<br />
is sclerosing adenosis.<br />
In rare cases sclerosing adenosis may<br />
be involved by DCIS or LIN {1046,<br />
1275a,1846a,2015,2336a,3104a}.<br />
Differential diagnosis<br />
S c l e rosing adenosis can mimic invasive<br />
c a rcinoma. The overall lobulated arc h i-<br />
t e c t u re, persistence of ME cells, and<br />
lack of epithelial atypia help to exclude<br />
<strong>carcinoma</strong> {321,1046}. In cases involved<br />
by in situ <strong>carcinoma</strong>, the immunohistochemical<br />
demonstration of persistent<br />
myoepithelial cells is crucial in excluding<br />
invasion.<br />
Benign epithelial proliferations<br />
81













