

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
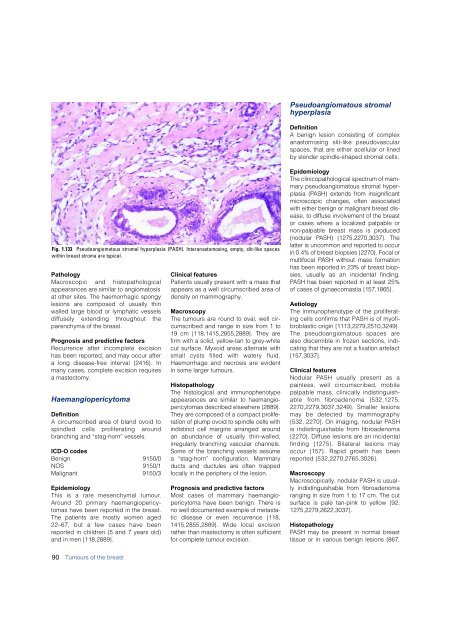
Pseudoangiomatous stromal<br />
hyperplasia<br />
Definition<br />
A benign lesion consisting of complex<br />
anastomosing slit-like pseudovascular<br />
spaces, that are either acellular or lined<br />
by slender spindle-shaped stromal cells.<br />
Fig. 1.133 Pseudoangiomatous stromal hyperplasia (PASH). Interanastomosing, empty, slit-like spaces<br />
within <strong>breast</strong> stroma are typical.<br />
Pathology<br />
M a c roscopic and histopathological<br />
appearances are similar to angiomatosis<br />
at other sites. The haemorrhagic spongy<br />
lesions are composed of usually thin<br />
walled large blood or lymphatic vessels<br />
d i ffusely extending throughout the<br />
parenchyma of the <strong>breast</strong>.<br />
Prognosis and predictive factors<br />
R e c u r rence after incomplete excision<br />
has been reported, and may occur after<br />
a long disease-free interval {2416}. In<br />
many cases, complete excision requires<br />
a mastectomy.<br />
Haemangiopericytoma<br />
Definition<br />
A circumscribed area of bland ovoid to<br />
spindled cells proliferating aro u n d<br />
branching and “stag-horn” vessels.<br />
ICD-O codes<br />
Benign 9150/0<br />
NOS 9150/1<br />
Malignant 9150/3<br />
Epidemiology<br />
This is a rare mesenchymal tumour.<br />
A round 20 primary haemangiopericytomas<br />
have been reported in the <strong>breast</strong>.<br />
The patients are mostly women aged<br />
22–67, but a few cases have been<br />
reported in children (5 and 7 years old)<br />
and in men {118,2889}.<br />
Clinical features<br />
Patients usually present with a mass that<br />
appears as a well circumscribed area of<br />
density on mammography.<br />
Macroscopy<br />
The tumours are round to oval, well circumscribed<br />
and range in size from 1 to<br />
19 cm {118,1415,2855,2889}. They are<br />
firm with a solid, yellow-tan to grey-white<br />
cut surface. Myxoid areas alternate with<br />
small cysts filled with watery fluid.<br />
Haemorrhage and necrosis are evident<br />
in some larger tumours.<br />
Histopathology<br />
The histological and immunophenotype<br />
appearances are similar to haemangiopericytomas<br />
described elsewhere {2889}.<br />
They are composed of a compact pro l i f e-<br />
ration of plump ovoid to spindle cells with<br />
indistinct cell margins arranged aro u n d<br />
an abundance of usually thin-walled,<br />
i r regularly branching vascular channels.<br />
Some of the branching vessels assume<br />
a “stag-horn” configuration. Mammary<br />
ducts and ductules are often trapped<br />
focally in the periphery of the lesion.<br />
Prognosis and predictive factors<br />
Most cases of mammary haemangiopericytoma<br />
have been benign. There is<br />
no well documented example of metastatic<br />
disease or even re c u r rence {118,<br />
1415,2855,2889}. Wide local excision<br />
rather than mastectomy is often sufficient<br />
for complete tumour excision.<br />
Epidemiology<br />
The clinicopathological spectrum of mamm<br />
a ry pseudoangiomatous stromal hyperplasia<br />
(PASH) extends from insignificant<br />
m i c roscopic changes, often associated<br />
with either benign or malignant <strong>breast</strong> disease,<br />
to diffuse involvement of the bre a s t<br />
or cases where a localized palpable or<br />
non-palpable <strong>breast</strong> mass is pro d u c e d<br />
(nodular PASH) {1275,2270,3037}. The<br />
latter is uncommon and re p o rted to occur<br />
in 0.4% of <strong>breast</strong> biopsies {2270}. Focal or<br />
multifocal PASH without mass form a t i o n<br />
has been re p o rted in 23% of <strong>breast</strong> biopsies,<br />
usually as an incidental finding.<br />
PASH has been re p o rted in at least 25%<br />
of cases of gynaecomastia {157,1865}.<br />
Aetiology<br />
The immunophenotype of the proliferating<br />
cells confirms that PASH is of myofibroblastic<br />
origin {1113,2279,2510,3249}.<br />
The pseudoangiomatous spaces are<br />
also discernible in frozen sections, indicating<br />
that they are not a fixation artefact<br />
{157,3037}.<br />
Clinical features<br />
Nodular PASH usually present as a<br />
painless, well circumscribed, mobile<br />
palpable mass, clinically indistinguishable<br />
from fibroadenoma {532,1275,<br />
2270,2279,3037,3249}. Smaller lesions<br />
may be detected by mammography<br />
{532, 2270}. On imaging, nodular PA S H<br />
is indistinguishable from fibro a d e n o m a<br />
{2270}. Diffuse lesions are an incidental<br />
finding {1275}. Bilateral lesions may<br />
occur {157}. Rapid growth has been<br />
re p o rted {532,2270,2765,3026}.<br />
Macroscopy<br />
Macroscopically, nodular PASH is usually<br />
indistinguishable from fibroadenoma<br />
ranging in size from 1 to 17 cm. The cut<br />
surface is pale tan-pink to yellow {92,<br />
1275,2279,2622,3037}.<br />
Histopathology<br />
PASH may be present in normal bre a s t<br />
tissue or in various benign lesions {867,<br />
90 Tumours of the <strong>breast</strong>













