

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
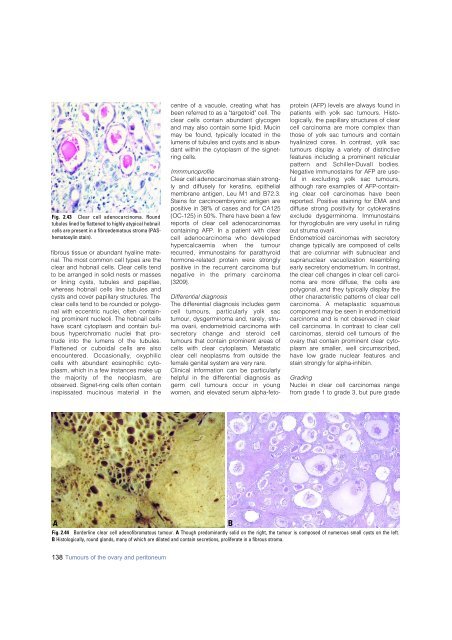
Fig. 2.43 Clear cell adeno<strong>carcinoma</strong>. Round<br />
tubules lined by flattened to highly atypical hobnail<br />
cells are present in a fibroedematous stroma (PAShematoxylin<br />
stain).<br />
fibrous tissue or abundant hyaline material.<br />
The most common cell types are the<br />
clear and hobnail cells. Clear cells tend<br />
to be arranged in solid nests or masses<br />
or lining cysts, tubules and papillae,<br />
whereas hobnail cells line tubules and<br />
cysts and cover papillary structures. The<br />
clear cells tend to be rounded or polygonal<br />
with eccentric nuclei, often containing<br />
prominent nucleoli. The hobnail cells<br />
have scant cytoplasm and contain bulbous<br />
hyperc h romatic nuclei that protrude<br />
into the lumens of the tubules.<br />
Flattened or cuboidal cells are also<br />
e n c o u n t e red. Occasionally, oxyphilic<br />
cells with abundant eosinophilic cytoplasm,<br />
which in a few instances make up<br />
the majority of the neoplasm, are<br />
observed. Signet-ring cells often contain<br />
inspissated mucinous material in the<br />
centre of a vacuole, creating what has<br />
been referred to as a "targetoid" cell. The<br />
clear cells contain abundant glycogen<br />
and may also contain some lipid. Mucin<br />
may be found, typically located in the<br />
lumens of tubules and cysts and is abundant<br />
within the cytoplasm of the signetring<br />
cells.<br />
Immmunoprofile<br />
Clear cell adeno<strong>carcinoma</strong>s stain strongly<br />
and diffusely for keratins, epithelial<br />
membrane antigen, Leu M1 and B72.3.<br />
Stains for carcinoembryonic antigen are<br />
positive in 38% of cases and for CA125<br />
(OC-125) in 50%. There have been a few<br />
reports of clear cell adeno<strong>carcinoma</strong>s<br />
containing AFP. In a patient with clear<br />
cell adeno<strong>carcinoma</strong> who developed<br />
h y p e rcalcaemia when the tumour<br />
recurred, immunostains for parathyroid<br />
h o rm o n e - related protein were stro n g l y<br />
positive in the recurrent <strong>carcinoma</strong> but<br />
negative in the primary carc i n o m a<br />
{3209}.<br />
Differential diagnosis<br />
The differential diagnosis includes germ<br />
cell tumours, particularly yolk sac<br />
tumour, dysgerminoma and, rarely, struma<br />
ovarii, endometrioid <strong>carcinoma</strong> with<br />
s e c re t o ry change and steroid cell<br />
tumours that contain prominent areas of<br />
cells with clear cytoplasm. Metastatic<br />
clear cell neoplasms from outside the<br />
female genital system are very rare.<br />
Clinical information can be particularly<br />
helpful in the differential diagnosis as<br />
g e rm cell tumours occur in young<br />
women, and elevated serum alpha-fetoprotein<br />
(AFP) levels are always found in<br />
patients with yolk sac tumours. Histologically,<br />
the papillary structures of clear<br />
cell <strong>carcinoma</strong> are more complex than<br />
those of yolk sac tumours and contain<br />
hyalinized cores. In contrast, yolk sac<br />
tumours display a variety of distinctive<br />
features including a prominent reticular<br />
p a t t e rn and Schiller-Duvall bodies.<br />
Negative immunostains for AFP are useful<br />
in excluding yolk sac tumours,<br />
although rare examples of AFP-containing<br />
clear cell <strong>carcinoma</strong>s have been<br />
reported. Positive staining for EMA and<br />
diffuse strong positivity for cytokeratins<br />
exclude dysgerminoma. Immunostains<br />
for thyroglobulin are very useful in ruling<br />
out struma ovarii.<br />
Endometrioid <strong>carcinoma</strong>s with secretory<br />
change typically are composed of cells<br />
that are columnar with subnuclear and<br />
supranuclear vacuolization re s e m b l i n g<br />
early secretory endometrium. In contrast,<br />
the clear cell changes in clear cell <strong>carcinoma</strong><br />
are more diffuse, the cells are<br />
polygonal, and they typically display the<br />
other characteristic patterns of clear cell<br />
c a rcinoma. A metaplastic squamous<br />
component may be seen in endometrioid<br />
<strong>carcinoma</strong> and is not observed in clear<br />
cell <strong>carcinoma</strong>. In contrast to clear cell<br />
<strong>carcinoma</strong>s, steroid cell tumours of the<br />
ovary that contain prominent clear cytoplasm<br />
are smaller, well circumscribed,<br />
have low grade nuclear features and<br />
stain strongly for alpha-inhibin.<br />
Grading<br />
Nuclei in clear cell <strong>carcinoma</strong>s range<br />
from grade 1 to grade 3, but pure grade<br />
A<br />
B<br />
Fig. 2.44 Borderline clear cell adenofibromatous tumour. A Though predominantly solid on the right, the tumour is composed of numerous small cysts on the left.<br />
B Histologically, round glands, many of which are dilated and contain secretions, proliferate in a fibrous stroma.<br />
138 Tumours of the ovary and peritoneum













