

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Secondary tumours of the uterine<br />
corpus<br />
V. Abeler<br />
U. Haller<br />
Definition<br />
Tumours of the uterine corpus that originate<br />
from, but are discontinuous with, a<br />
primary extrauterine tumour or a tumour<br />
in the cervix or elsewhere in the uterus.<br />
Clinical features<br />
Signs and symptoms<br />
The mean age of patients with extragenital<br />
tumour metastasis to the uterus is 60<br />
years. Patients have abnormal uterine<br />
bleeding since most neoplasms metastatic<br />
to the uterus infiltrate the endometrium<br />
diffusely.<br />
Imaging<br />
Imaging studies are non-specific {1240,<br />
1282,1576,3184}.<br />
Macroscopy<br />
Metastases may appear as solitary or<br />
multiple tumours or be diffusely infiltrating.<br />
Histopathology<br />
The majority of metastases to the uterus<br />
a re confined to the myometrium.<br />
However, approximately one-third involve<br />
the endometrium and thus can be<br />
detected in biopsy specimens {1529}.<br />
Metastatic <strong>carcinoma</strong> within the<br />
endometrium and/or myometrium characteristically<br />
infiltrates as single cells,<br />
cord or glands. The appearance is particularly<br />
striking in lobular <strong>carcinoma</strong> of<br />
the <strong>breast</strong>, which usually retains its single-file<br />
pattern, and with metastatic<br />
signet-ring cell <strong>carcinoma</strong> of the stomach<br />
or colon. Metastatic colon <strong>carcinoma</strong><br />
of the usual type may form large tumour<br />
masses and can mimic an endometrial<br />
<strong>carcinoma</strong> of mucinous or endometrioid<br />
type.<br />
Metastatic <strong>carcinoma</strong> in the endometrium<br />
should be suspected if one or more<br />
of the following features are pre s e n t<br />
{1539}.<br />
(1) A tumour with an unusual macroscopic<br />
or histological pattern for primary<br />
endometrial <strong>carcinoma</strong>.<br />
(2) Diffuse replacement by tumour of<br />
endometrial stroma with sparing of occasional<br />
normal endometrial glands.<br />
(3) Lack of premalignant changes in<br />
endometrial glands.<br />
(4) Lack of tumour necrosis<br />
For specific identification of certain prim<br />
a ry tumours immunohistochemical<br />
studies are frequently required.<br />
Origin and histogenesis<br />
In most instances the primary tumour is<br />
well known, or disseminated disease is<br />
clinical evident. Occasionally, a tumour<br />
diagnosed by curettage or hysterectomy<br />
represents the first sign of an extrauterine<br />
primary tumour.<br />
Secondary tumours of the uterine corpus<br />
can be divided into two major groups:<br />
tumours of the genital and extragenital<br />
organs. Neoplasms of neighbouring<br />
organs such as cervix, fallopian tubes,<br />
ovaries, bladder and rectum can metastasize<br />
to the uterine corpus via lymphatics<br />
or blood vessels but mostly represent<br />
local direct extension.<br />
Haematogenous or lymphatic uterine<br />
metastases from any extragenital primary<br />
tumour may occur but are extremely<br />
rare. Reported primary tumours<br />
include <strong>carcinoma</strong>s of the <strong>breast</strong>, stomach,<br />
colon, pancreas, gallbladder, lung,<br />
u r i n a ry bladder and thyroid and<br />
melanoma {192,1452,1455,1529,1531,<br />
1620,1720}. Mammary lobular <strong>carcinoma</strong>,<br />
gastric signet-ring cell <strong>carcinoma</strong><br />
and colonic <strong>carcinoma</strong> are the most frequently<br />
re p o rted extragenital primary<br />
tumours {1529,1531}.<br />
Prognosis and predictive factors<br />
When uterine metastases are present,<br />
the patient usually has widely disseminated<br />
disease. However, in one series<br />
the average survival was 20 months after<br />
the diagnosis of uterine metastases. The<br />
reason for this relatively favourable outcome<br />
might be the predominance of<br />
cases of metastatic <strong>breast</strong> <strong>carcinoma</strong><br />
{1529}.<br />
A<br />
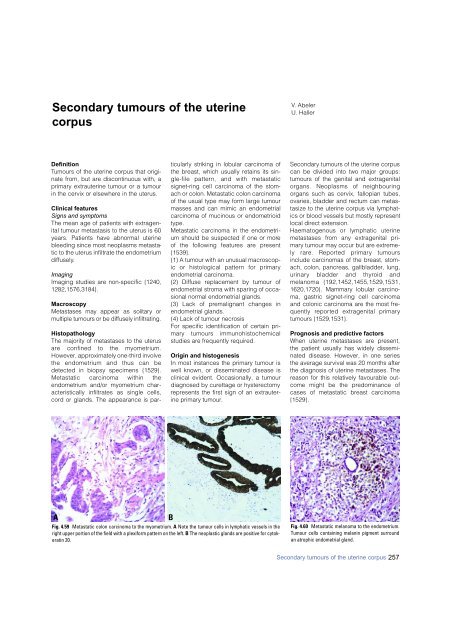
Fig. 4.59 Metastatic colon <strong>carcinoma</strong> to the myometrium. A Note the tumour cells in lymphatic vessels in the<br />
right upper portion of the field with a plexiform pattern on the left. B The neoplastic glands are positive for cytokeratin<br />
20.<br />
B<br />
Fig. 4.60 Metastatic melanoma to the endometrium.<br />
Tumour cells containing melanin pigment surround<br />
an atrophic endometrial gland.<br />
Secondary tumours of the uterine corpus 257













