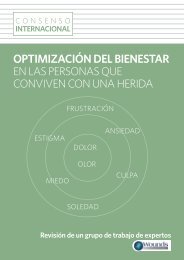
NEGATIVE PRESSURE WOUND THERAPY IN DIABETIC FOOT WOUNDS ■ 115betic feet without ischemia. A range of advantageswas demonstrated when comparedwith conventional therapy (saline gauzealone), and includes improvements in thespeed of granulation tissue formation,decrease in wound dimensions, time to healing,cost of treatment and rate of amputations.In general, an improved chance of fasterhealing with grade 1 diabetic foot ulcers isobserved with the application of NPWT,which may not be immediately warranted inthese wounds (19).Certain wound types may benefit moresignificantly from application of NPWT thanothers, as is the case of larger and olderwounds (more than one year in duration),which are less likely to achieve a positive outcomewith conventional therapy. When thesewounds are treated with NPWT, their ratesof healing are closer to the results obtainedwith the smaller and more recent wounds(20).With respect to the duration of NPWT,several publications favour wound closure bysecondary intention (21, 22) (Figure 2), sinceFigure 2. Wound resulting from amputation of the 3 first toes: 4 days after the surgery (A); 30 days aftersurgery and 25 after the beginning of NPWT (B); 5 months later, secondary intention healed wound (C).it has been shown to improve the rate of closureand reduce the time to healing. However,the use of NPWT until complete wound closure,which lasts for a relatively long period oftreatment, has an important impact on thepatient’s quality of life and overall cost of therapy.Therefore, NPWT can also be used as abridge to surgical grafting (23), increasing thespeed of granulation tissue formation until thewound becomes a good candidate to receive askin graft. This strategy may reduce the lengthof hospital stay and the cost of therapy.Ischemic foot ulcersMost published studies regarding diabeticfoot ulcers describe results following NPWTin adequately perfused limbs. However, it iswell recognized that diabetic patients typicallyhave tibial and peroneal arterial occlusivedisease and ischemia results from atheroscleroticmacrovascular disease besides themicrocirculatory dysfunction (24). The use ofNPWT on ischemic limb wounds is a highlyspecialized clinical scenario since in theabsence of adequate blood perfusion, normalwound healing process cannot proceed (25).Therefore, revascularization is undoubtedlythe best intervention to achieve limb salvagein patients with limb ischemia.After successful revascularization, NPWTmay be considered as an advanced woundcare therapy for lower limb ulcerations (18).In such cases, it has demonstrated to signifi-
116 ■ PIE DIABÉTICOcantly improve healing outcomes in both arte -rial ulcers (26, 27) and minor amputationstumps (28, 29). However, in up to 14% of patients,revascularization procedures are notrecommended for technical or clinical reasons(30), and even when such procedures can beperformed, they will fail in a significant proportionof cases (31). No<strong>net</strong>heless, it has beenshown that the majority of limbs with criticallimb ischemia not suitable for revascularisationcan be salvaged. In this situation, NPWT can beused with the goal of preventing amputationsince several studies have reported completehealing of wounds following NPWT in patientswith critical limb ischemia in the absence ofsuccessful revascularisation (32, 33).Infected ulcersInfection is a well-recognised barrier towound healing, which often requires systemicantibiotic therapy and surgical debridement ofinfected or necrotic tissue. NPWT should beused only as an adjunctive therapy to controlinfection and never as a substitute of suchmeasures. Despite reporting either no reductionor increasing in bacterial numbers, severalstudies identified a favourable response ofwounds to NPWT (34, 35) while othersreported even a higher rate of resolution ofclinically apparent infection in wounds treatedwith NPWT compared to alternative means(36). Such observations can be explained bythe beneficial effects of NPWT on woundhealing, which include control of oedema,increased perfusion, wound contraction andgranulation tissue formation.Wound fillers with active anti-microbialproperties like anti-microbial gauze may contributetowards infection control and silverfoam and anti-microbial WCL may, as well,have a similar effect.Contraindications to the useof Negative Pressure Wound TherapyAs previously mentioned, NPWT cannotbe considered a substitute for surgicaldebridement and its application is contraindicatedin wounds containing necrotic tissue(37). In case of infected wounds, regulatorybodies recommend careful considerationbefore NPWT is applied, and its use inuntreated osteomyelitis is contraindicated(37). The application of NPWT onto exposedorgans, exposed vasculature or anastomoticsites is also contra-indicated (18).TREATMENT VARIABLESFOR NEGATIVE PRESSUREWOUND THERAPYWound filler and wound contact layerThe wound filler is the material used to fillthe wound and is most commonly composedof polyurethane (PU) «black» foam andpolyvinyl alcohol (PVA) «white» foam orgauze. The wound filler can be directly appliedon the wound bed or used in conjunctionwith a wound contact layer (WCL) that is a thinlayer of material between the wound bed (andsometimes the surrounding skin) and theNPWT wound filler. Different wound fillersand WCL may determine a different tissueresponse to NPWT and that is why suchmaterials must be selected according to thetype of wound.No differences in the degree of blood flow(38) or wound contraction in small wounds(39, 40) have been observed with either foamor gauze, although PU foam results in morecontraction than gauze in large wounds (41). Interms of clinical outcomes, the rate of reductionof wound size (42) and the healing time(34) seem to be similar with both wound fillers.PU foam promotes rapid and thick granulationtissue formation (5, 43) whereas PVAfoam (5) and gauze (43) are thought to formthinner but more stable granulation tissue.Moreover, PU foam is responsible for a higherlevel of tissue ingrowth when comparedwith gauze (44). Removal of the foam alongwith the ingrown tissue causes tissue damageand bleeding, being painful for the patient(45). Therefore, gauze and possibly PVA foamshould be considered to reduce patient’s pain