

Instructions for use: Ikus - Berlin Heart
Instructions for use: Ikus - Berlin Heart
Instructions for use: Ikus - Berlin Heart

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
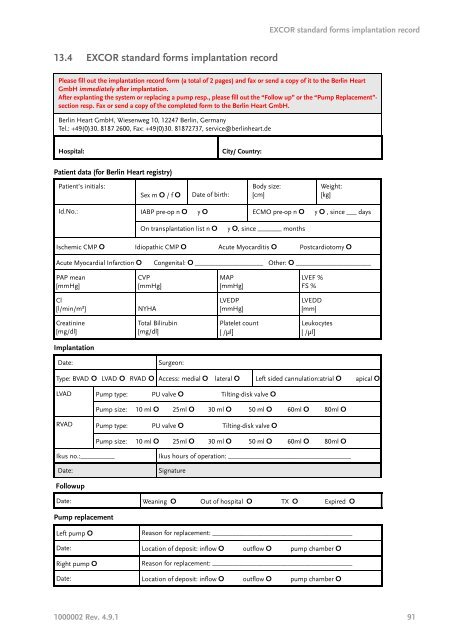
13.4 EXCOR standard <strong>for</strong>ms implantation record<br />
EXCOR standard <strong>for</strong>ms implantation record<br />
Please fill out the implantation record <strong>for</strong>m (a total of 2 pages) and fax or send a copy of it to the <strong>Berlin</strong> <strong>Heart</strong><br />
GmbH immediately after implantation.<br />
After explanting the system or replacing a pump resp., please fill out the “Follow up” or the “Pump Replacement”section<br />
resp. Fax or send a copy of the completed <strong>for</strong>m to the <strong>Berlin</strong> <strong>Heart</strong> GmbH.<br />
<strong>Berlin</strong> <strong>Heart</strong> GmbH, Wiesenweg 10, 12247 <strong>Berlin</strong>, Germany<br />
Tel.: +49(0)30. 8187 2600, Fax: +49(0)30. 81872737, service@berlinheart.de<br />
Hospital: City/ Country:<br />
Patient data (<strong>for</strong> <strong>Berlin</strong> <strong>Heart</strong> registry)<br />
Patient’s initials:<br />
Implantation<br />
Followup<br />
Pump replacement<br />
Sex m O / f O Date of birth:<br />
Body size:<br />
[cm]<br />
Weight:<br />
[kg]<br />
Id.No.: IABP pre-op n O y O ECMO pre-op n O y O , since ___ days<br />
On transplantation list n O y O, since _______ months<br />
Ischemic CMP O Idiopathic CMP O Acute Myocarditis O Postcardiotomy O<br />
Acute Myocardial Infarction O Congenital: O ____________________ Other: O ______________________<br />
PAP mean<br />
[mmHg]<br />
CVP<br />
[mmHg]<br />
Cl<br />
[l/min/m²] NYHA<br />
Creatinine<br />
[mg/dl]<br />
Total Bilirubin<br />
[mg/dl]<br />
Date: Surgeon:<br />
MAP<br />
[mmHg]<br />
LVEDP<br />
[mmHg]<br />
Platelet count<br />
[ /μl]<br />
LVEF %<br />
FS %<br />
LVEDD<br />
[mm]<br />
Leukocytes<br />
[ /μl]<br />
Type: BVAD O LVAD O RVAD O Access: medial O lateral O Left sided cannulation:atrial O apical O<br />
LVAD Pump type: PU valve O Tilting-disk valve O<br />
Pump size: 10 ml O 25ml O 30 ml O 50 ml O 60ml O 80ml O<br />
RVAD Pump type: PU valve O Tilting-disk valve O<br />
Pump size: 10 ml O 25ml O 30 ml O 50 ml O 60ml O 80ml O<br />
<strong>Ikus</strong> no.:__________ <strong>Ikus</strong> hours of operation: ____________________________________<br />
Date: Signature<br />
Date: Weaning O Out of hospital O TX O Expired O<br />
Left pump O Reason <strong>for</strong> replacement: _________________________________________<br />
Date: Location of deposit: inflow O outflow O pump chamber O<br />
Right pump O Reason <strong>for</strong> replacement: _________________________________________<br />
Date: Location of deposit: inflow O outflow O pump chamber O<br />
1000002 Rev. 4.9.1 91




