Techniques d'ablation de l'endomètre dans le traitement ... - INESSS
Techniques d'ablation de l'endomètre dans le traitement ... - INESSS
Techniques d'ablation de l'endomètre dans le traitement ... - INESSS

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
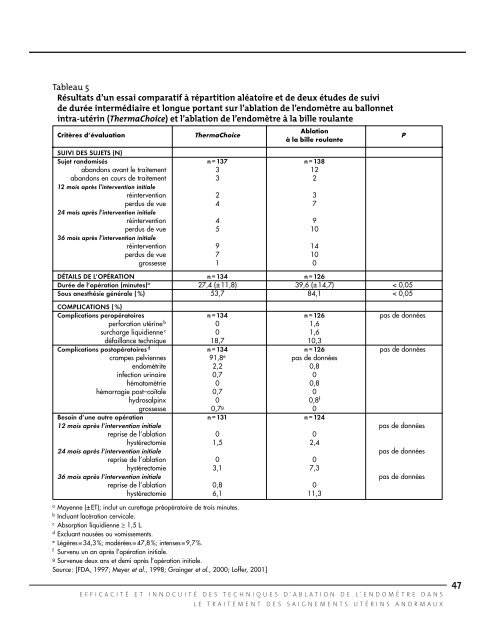
Tab<strong>le</strong>au 5<br />
Résultats d’un essai comparatif à répartition aléatoire et <strong>de</strong> <strong>de</strong>ux étu<strong>de</strong>s <strong>de</strong> suivi<br />
<strong>de</strong> durée intermédiaire et longue portant sur l’ablation <strong>de</strong> l’endomètre au ballonnet<br />
intra-utérin (ThermaChoice) et l’ablation <strong>de</strong> l’endomètre à la bil<strong>le</strong> roulante<br />
Critères d’évaluation ThermaChoice<br />
Ablation<br />
à la bil<strong>le</strong> roulante<br />
SUIVI DES SUJETS (N)<br />
Sujet randomisés n=137 n =138<br />
abandons avant <strong>le</strong> <strong>traitement</strong> 3 12<br />
abandons en cours <strong>de</strong> <strong>traitement</strong> 3 2<br />
12 mois après l’intervention initia<strong>le</strong><br />
réintervention 2 3<br />
perdus <strong>de</strong> vue 4 7<br />
24 mois après l’intervention initia<strong>le</strong><br />
réintervention 4 9<br />
perdus <strong>de</strong> vue 5 10<br />
36 mois après l’intervention initia<strong>le</strong><br />
réintervention 9 14<br />
perdus <strong>de</strong> vue 7 10<br />
grossesse 1 0<br />
DÉTAILS DE L’OPÉRATION n=134 n=126<br />
Durée <strong>de</strong> l’opération (minutes) a 27,4 (±11,8) 39,6 (±14,7) < 0,05<br />
Sous anesthésie généra<strong>le</strong> (%) 53,7 84,1 < 0,05<br />
COMPLICATIONS (%)<br />
Complications peropératoires n=134 n=126 pas <strong>de</strong> données<br />
perforation utérine b 0 1,6<br />
surcharge liquidienne c 0 1,6<br />
défaillance technique 18,7 10,3<br />
Complications postopératoires d n=134 n=126 pas <strong>de</strong> données<br />
crampes pelviennes 91,8 e pas <strong>de</strong> données<br />
endométrite 2,2 0,8<br />
infection urinaire 0,7 0<br />
hématométrie 0 0,8<br />
hémorragie post–coïta<strong>le</strong> 0,7 0<br />
hydrosalpinx 0 0,8 f<br />
grossesse 0,7 g 0<br />
Besoin d’une autre opération n =131 n =124<br />
12 mois après l’intervention initia<strong>le</strong> pas <strong>de</strong> données<br />
reprise <strong>de</strong> l’ablation 0 0<br />
hystérectomie 1,5 2,4<br />
24 mois après l’intervention initia<strong>le</strong> pas <strong>de</strong> données<br />
reprise <strong>de</strong> l’ablation 0 0<br />
hystérectomie 3,1 7,3<br />
36 mois après l’intervention initia<strong>le</strong> pas <strong>de</strong> données<br />
reprise <strong>de</strong> l’ablation 0,8 0<br />
hystérectomie 6,1 11,3<br />
a Moyenne (±ET); inclut un curettage préopératoire <strong>de</strong> trois minutes.<br />
b Incluant lacération cervica<strong>le</strong>.<br />
c Absorption liquidienne ≥ 1,5 L.<br />
d Excluant nausées ou vomissements.<br />
e Légères =34,3 %; modérées =47,8 %; intenses =9,7 %.<br />
f Survenu un an après l’opération initia<strong>le</strong>.<br />
g Survenue <strong>de</strong>ux ans et <strong>de</strong>mi après l’opération initia<strong>le</strong>.<br />
Source : [FDA, 1997; Meyer et al., 1998; Grainger et al., 2000; Loffer, 2001]<br />
EFFICACITÉ ET INNOCUITÉ DES TECHNIQUES D'ABLATION DE L'ENDOMÈTRE DANS<br />
LE TRAITEMENT DES SAIGNEMENTS UTÉRINS ANORMAUX<br />
P<br />
47