30845 Suppl Giot.pdf - Giornale Italiano di Ortopedia e Traumatologia
30845 Suppl Giot.pdf - Giornale Italiano di Ortopedia e Traumatologia
30845 Suppl Giot.pdf - Giornale Italiano di Ortopedia e Traumatologia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
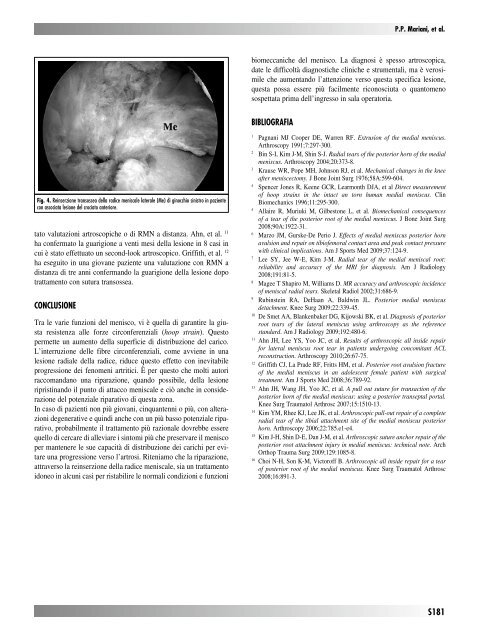
Fig. 4. Reinserzione transossea della ra<strong>di</strong>ce meniscale laterale (Me) <strong>di</strong> ginocchio sinistro in paziente<br />
con associata lesione del crociato anteriore.<br />
tato valutazioni artroscopiche o <strong>di</strong> RMN a <strong>di</strong>stanza. Ahn, et al. 11<br />
ha confermato la guarigione a venti mesi della lesione in 8 casi in<br />
cui è stato effettuato un second-look artroscopico. Griffith, et al. 12<br />
ha eseguito in una giovane paziente una valutazione con RMN a<br />
<strong>di</strong>stanza <strong>di</strong> tre anni confermando la guarigione della lesione dopo<br />
trattamento con sutura transossea.<br />
CONCLuSIONE<br />
Tra le varie funzioni del menisco, vi è quella <strong>di</strong> garantire la giusta<br />
resistenza alle forze circonferenziali (hoop strain). Questo<br />
permette un aumento della superficie <strong>di</strong> <strong>di</strong>stribuzione del carico.<br />
L’interruzione delle fibre circonferenziali, come avviene in una<br />
lesione ra<strong>di</strong>ale della ra<strong>di</strong>ce, riduce questo effetto con inevitabile<br />
progressione dei fenomeni artritici. È per questo che molti autori<br />
raccomandano una riparazione, quando possibile, della lesione<br />
ripristinando il punto <strong>di</strong> attacco meniscale e ciò anche in considerazione<br />
del potenziale riparativo <strong>di</strong> questa zona.<br />
In caso <strong>di</strong> pazienti non più giovani, cinquantenni o più, con alterazioni<br />
degenerative e quin<strong>di</strong> anche con un più basso potenziale riparativo,<br />
probabilmente il trattamento più razionale dovrebbe essere<br />
quello <strong>di</strong> cercare <strong>di</strong> alleviare i sintomi più che preservare il menisco<br />
per mantenere le sue capacità <strong>di</strong> <strong>di</strong>stribuzione dei carichi per evitare<br />
una progressione verso l’artrosi. Riteniamo che la riparazione,<br />
attraverso la reinserzione della ra<strong>di</strong>ce meniscale, sia un trattamento<br />
idoneo in alcuni casi per ristabilire le normali con<strong>di</strong>zioni e funzioni<br />
P.P. Mariani, et al.<br />
biomeccaniche del menisco. La <strong>di</strong>agnosi è spesso artroscopica,<br />
date le <strong>di</strong>fficoltà <strong>di</strong>agnostiche cliniche e strumentali, ma è verosimile<br />
che aumentando l’attenzione verso questa specifica lesione,<br />
questa possa essere più facilmente riconosciuta o quantomeno<br />
sospettata prima dell’ingresso in sala operatoria.<br />
BIBLIOGraFIa<br />
1 Pagnani MJ Cooper DE, Warren RF. Extrusion of the me<strong>di</strong>al meniscus.<br />
Arthroscopy 1991;7:297-300.<br />
2 Bin S-I, Kim J-M, Shin S-J. Ra<strong>di</strong>al tears of the posterior horn of the me<strong>di</strong>al<br />
meniscus. Arthroscopy 2004;20:373-8.<br />
3 Krause WR, Pope MH, Johnson RJ, et al. Mechanical changes in the knee<br />
after meniscectomy. J Bone Joint Surg 1976;58A:599-604.<br />
4 Spencer Jones R, Keene GCR, Learmonth DJA, et al Direct measurement<br />
of hoop strains in the intact an torn human me<strong>di</strong>al meniscus. Clin<br />
Biomechanics 1996;11:295-300.<br />
5 Allaire R, Muriuki M, Gilbestone L, et al. Biomechanical consequences<br />
of a tear of the posterior root of the me<strong>di</strong>al meniscus. J Bone Joint Surg<br />
2008;90A:1922-31.<br />
6 Marzo JM, Gurske-De Perio J. Effects of me<strong>di</strong>al meniscus posterior horn<br />
avulsion and repair on tibiofemoral contact area and peak contact pressure<br />
with clinical implications. Am J Sports Med 2009;37:124-9.<br />
7 Lee SY, Jee W-E, Kim J-M. Ra<strong>di</strong>al tear of the me<strong>di</strong>al meniscal root:<br />
reliability and accuracy of the MRI for <strong>di</strong>agnosis. Am J Ra<strong>di</strong>ology<br />
2008;191:81-5.<br />
8 Magee T Shapiro M, Williams D. MR accuracy and arthroscopic incidence<br />
of meniscal ra<strong>di</strong>al tears. Skeletal Ra<strong>di</strong>ol 2002;31:686-9.<br />
9 Rubinstein RA, DeHaan A, Baldwin JL. Posterior me<strong>di</strong>al meniscus<br />
detachment. Knee Surg 2009;22:339-45.<br />
10 De Smet AA, Blankenbaker DG, Kijowski BK, et al. Diagnosis of posterior<br />
root tears of the lateral meniscus using arthroscopy as the reference<br />
standard. Am J Ra<strong>di</strong>ology 2009;192:480-6.<br />
11 Ahn JH, Lee YS, Yoo JC, et al. Results of arthroscopic all inside repair<br />
for lateral meniscus root tear in patients undergoing concomitant ACL<br />
reconstruction. Arthroscopy 2010;26:67-75.<br />
12 Griffith CJ, La Prade RF, Fritts HM, et al. Posterior root avulsion fracture<br />
of the me<strong>di</strong>al meniscus in an adolescent female patient with surgical<br />
treatment. Am J Sports Med 2008;36:789-92.<br />
13 Ahn JH, Wang JH, Yoo JC, et al. A pull out suture for transaction of the<br />
posterior horn of the me<strong>di</strong>al meniscus: using a posterior transeptal portal.<br />
Knee Surg Traumatol Arthrosc 2007;15:1510-13.<br />
14 Kim YM, Rhee KJ, Lee JK, et al. Arthroscopic pull-out repair of a complete<br />
ra<strong>di</strong>al tear of the tibial attachment site of the me<strong>di</strong>al meniscus posterior<br />
horn. Arthroscopy 2006;22:785.e1-e4.<br />
15 Kim J-H, Shin D-E, Dan J-M, et al. Arthroscopic suture anchor repair of the<br />
posterior root attachment injury in me<strong>di</strong>al meniscus: technical note. Arch<br />
Orthop Trauma Surg 2009;129:1085-8.<br />
16 Choi N-H, Son K-M, Victoroff B. Arthroscopic all inside repair for a tear<br />
of posterior root of the me<strong>di</strong>al meniscus. Knee Surg Traumatol Arthrosc<br />
2008;16:891-3.<br />
S181